

The therapeutic potential of apelin in kidney disease
- PMID: 34389827
- PMCID: PMC8361827
- DOI: 10.1038/s41581-021-00461-z
The therapeutic potential of apelin in kidney disease
Abstract
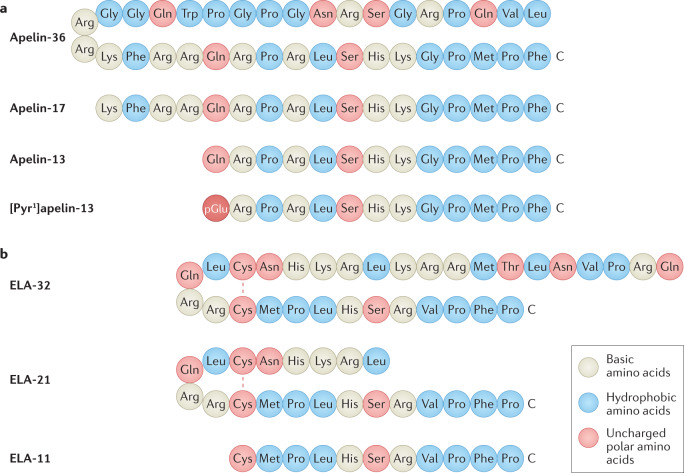
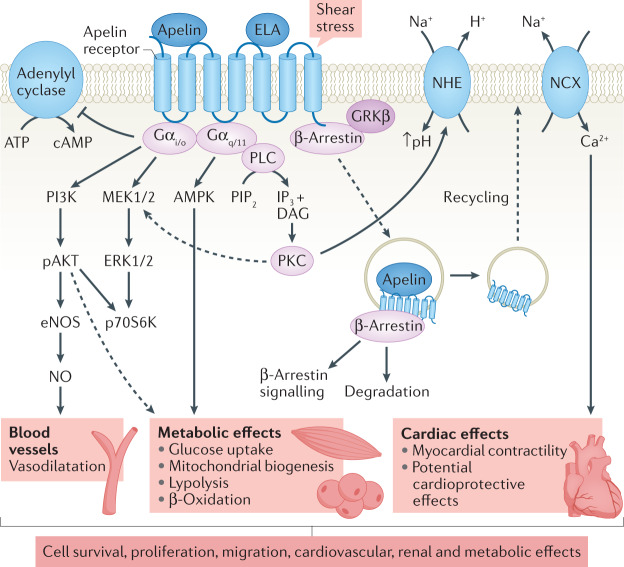
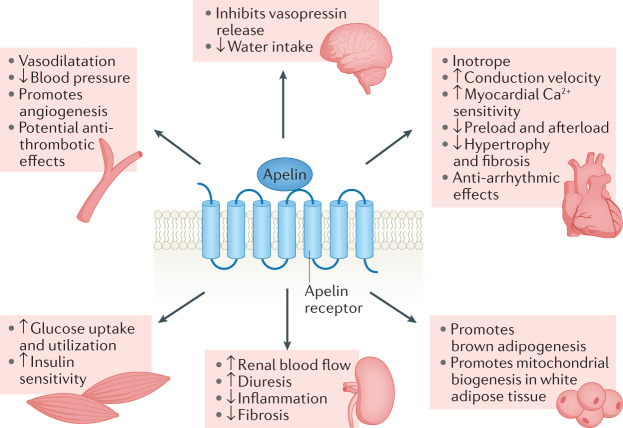
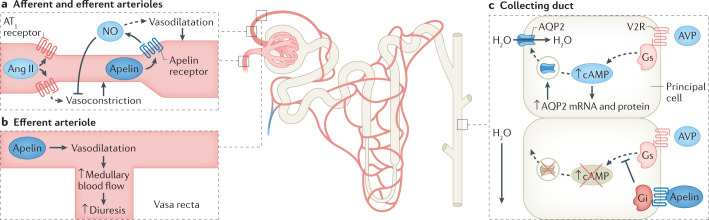
Chronic kidney disease (CKD) is a leading cause of global morbidity and mortality and is independently associated with cardiovascular disease. The mainstay of treatment for CKD is blockade of the renin-angiotensin-aldosterone system (RAAS), which reduces blood pressure and proteinuria and slows kidney function decline. Despite this treatment, many patients progress to kidney failure, which requires dialysis or kidney transplantation, and/or die as a result of cardiovascular disease. The apelin system is an endogenous physiological regulator that is emerging as a potential therapeutic target for many diseases. This system comprises the apelin receptor and its two families of endogenous ligands, apelin and elabela/toddler. Preclinical and clinical studies show that apelin receptor ligands are endothelium-dependent vasodilators and potent inotropes, and the apelin system has a reciprocal relationship with the RAAS. In preclinical studies, apelin regulates glomerular haemodynamics and acts on the tubule to promote aquaresis. In addition, apelin is protective in several kidney injury models. Although the apelin system has not yet been studied in patients with CKD, the available data suggest that apelin is a promising potential therapeutic target for kidney disease.
© 2021. Springer Nature Limited.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
