

Cost Effectiveness of a Cultural Physical Activity Intervention to Reduce Blood Pressure Among Native Hawaiians with Hypertension
- PMID: 34389923
- PMCID: PMC8807791
- DOI: 10.1007/s41669-021-00291-6
Cost Effectiveness of a Cultural Physical Activity Intervention to Reduce Blood Pressure Among Native Hawaiians with Hypertension
Abstract
Objective: The aim of this study was to calculate the costs and assess whether a culturally grounded physical activity intervention offered through community-based organizations is cost effective in reducing blood pressure among Native Hawaiian adults with hypertension.
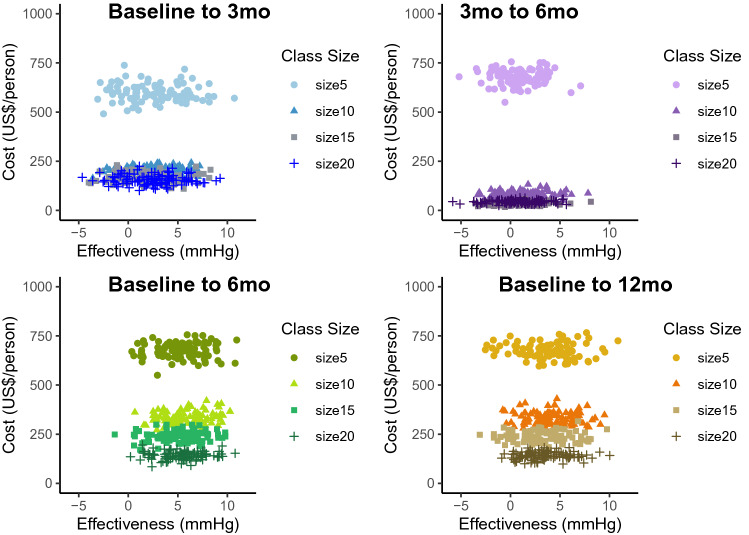
Methods: Six community-based organizations in Hawai'i completed a randomized controlled trial between 2015 and 2019. Overall, 263 Native Hawaiian adults with uncontrolled hypertension (≥ 140 mmHg systolic, ≥ 90 mmHg diastolic) were randomized to either a 12-month intervention group of hula (traditional Hawaiian dance) lessons and self-regulation classes, or to an education-only waitlist control group. The primary outcome was change in systolic blood pressure collected at baseline and 3, 6, and 12 months for the intervention compared with the control group. Incremental cost-effectiveness ratios (ICERs) were calculated for primary and secondary outcomes. Non-parametric bootstrapping and sensitivity analyses evaluated uncertainty in parameters and outcomes.
Results: The mean intervention cost was US$361/person, and the 6-month ICER was US$103/mmHg reduction in systolic blood pressure and US$95/mmHg in diastolic blood pressure. At 12 months, the intervention group maintained reductions in blood pressure, which exceeded reductions for usual care based on blood pressure outcomes. The change in blood pressure at 12 months resulted in ICERs of US$100/mmHg reduction in systolic blood pressure and US$93/mmHg in diastolic blood pressure. Sensitivity analyses suggested that at the estimated intervention cost, the probability that the program would lower systolic blood pressure by 5 mmHg was 67 and 2.5% at 6 and 12 months, respectively.
Conclusion: The 6-month Ola Hou program may be cost effective for low-resource community-based organizations. Maintenance of blood pressure reductions at 6 and 12 months in the intervention group contributed to potential cost effectiveness. Future studies should further evaluate the cost effectiveness of indigenous physical activity programs in similar settings and by modeling lifetime costs and quality-adjusted life-years.
Trial registration number: NCT02620709.
© 2021. The Author(s).
Conflict of interest statement
Ashley F. Railey, Clemma Muller, Carolyn Noonan, Maureen Schmitter-Edgecombe, Ka’imi Sinclair, Corin Kim, Mele Look, and J. Keawe‘aimoku Kaholokula have declared no conflicts of interest.
Figures

Similar articles
-
A Cultural Dance Program Improves Hypertension Control and Cardiovascular Disease Risk in Native Hawaiians: A Randomized Controlled Trial.Ann Behav Med. 2021 Oct 4;55(10):1006-1018. doi: 10.1093/abm/kaaa127. Ann Behav Med. 2021. PMID: 33677520 Free PMC article. Clinical Trial.
-
Kā-HOLO Project: a protocol for a randomized controlled trial of a native cultural dance program for cardiovascular disease prevention in Native Hawaiians.BMC Public Health. 2017 Apr 17;17(1):321. doi: 10.1186/s12889-017-4246-3. BMC Public Health. 2017. PMID: 28415975 Free PMC article. Clinical Trial.
-
Cultural Dance Program Improves Hypertension Management for Native Hawaiians and Pacific Islanders: a Pilot Randomized Trial.J Racial Ethn Health Disparities. 2017 Feb;4(1):35-46. doi: 10.1007/s40615-015-0198-4. Epub 2015 Dec 22. J Racial Ethn Health Disparities. 2017. PMID: 27294768 Free PMC article. Clinical Trial.
-
Behavioural modification interventions for medically unexplained symptoms in primary care: systematic reviews and economic evaluation.Health Technol Assess. 2020 Sep;24(46):1-490. doi: 10.3310/hta24460. Health Technol Assess. 2020. PMID: 32975190 Free PMC article.
-
Motivational support intervention to reduce smoking and increase physical activity in smokers not ready to quit: the TARS RCT.Health Technol Assess. 2023 Mar;27(4):1-277. doi: 10.3310/KLTG1447. Health Technol Assess. 2023. PMID: 37022933 Free PMC article.
Cited by
-
The Health Effects of a Cherokee Grounded Culture and Leadership Program.Int J Environ Res Public Health. 2022 Jun 30;19(13):8018. doi: 10.3390/ijerph19138018. Int J Environ Res Public Health. 2022. PMID: 35805678 Free PMC article.
References
-
- Tung WC, Barnes M. Heart diseases among Native Hawaiians and Pacific Islanders. Home Health Care Manag Pract. 2014;26:110–113.
-
- Johnson DB, Oyama N, LeMarchand L, Wilkens L. Native Hawaiians mortality, morbidity, and lifestyle: comparing data from 1982, 1990, and 2000. Pac Health Dialogues. 2004;11:120–130. - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
