

Patient monitoring across the spectrum of heart failure disease management 10 years after the CHAMPION trial
- PMID: 34390219
- PMCID: PMC8497370
- DOI: 10.1002/ehf2.13550
Patient monitoring across the spectrum of heart failure disease management 10 years after the CHAMPION trial
Abstract
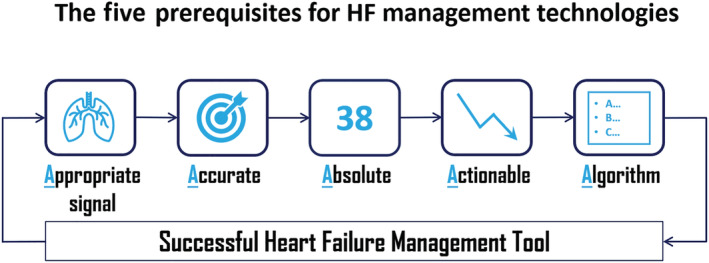
Despite significant advances in drug-based and device-based therapies, heart failure remains a major and growing public health problem associated with substantial disability, frequent hospitalizations, and high economic costs. Keeping patients well and out of the hospital has become a major focus of heart failure disease management. Achieving and maintaining such stability in heart failure patients requires a holistic approach, which includes at least the management of the underlying heart disease, the management of comorbidities and the social and psychological aspects of the disease, and the management of haemodynamic/fluid status. In this regard, accurate assessment of elevated ventricular filling pressures or volume overload, that is, haemodynamic or pulmonary congestion, respectively, before the onset of worsening heart failure symptoms represents an important management strategy. Unfortunately, conventional methods for assessing congestion, such as physical examination and monitoring of symptoms and daily weights, are insensitive markers of worsening heart failure. Assessment tools that directly measure congestion, accurately and in absolute terms, provide more actionable information that enables the application of treatment algorithms designed to restore patient stability, in a variety of clinical settings. Two such assessment tools, implantable haemodynamic monitors and remote dielectric sensing (ReDS), meet the prerequisites for useful heart failure management tools, by providing accurate, absolute, and actionable measures of congestion, to guide patient management. This review focuses on the use of such technologies, across the spectrum of heart failure treatment settings. Clinical data are presented that support the broad use of pulmonary artery pressure-guided and/or ReDS-guided heart failure management in heart failure patients with reduced and preserved left ventricular ejection fraction.
Keywords: Heart failure management; Lung fluid; Pulmonary pressure; Remote monitoring.
© 2021 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
WTA: Dr Abraham has received consulting fees from Abbott, Sensible Medical Innovations, Ltd., and Vectorious Medical Technologies. DB: Dr Bensimhon has received consulting fees from Sensible Medical Innovations, Ltd. SPP: Dr Pinney has received consulting fees from Abbott. SCF: Dr Feitell has received consulting fees from Abbott and Sensible Medical Innovations, Ltd. WFP: Dr Peacock has received consulting fees from Abbott. OA: Dr Amir has received consulting fees from Sensible Medical Innovations, Ltd. DB: Dr Burkhoff declares no relevant disclosures.
Figures
References
-
- Lund LH, Rich MW, Hauptman PJ. Complexities of the global heart failure epidemic. J Card Fail 2018; 24: 813–814. - PubMed
-
- Ambrosy AP, Fonarow GC, Butler J, Chioncel O, Greene SJ, Vaduganathan M, Nodari S, Lam CSP, Sato N, Shah AN, Gheorghiade M. The global health and economic burden of hospitalizations for heart failure: lessons learned from hospitalized heart failure registries. J Am Coll Cardiol 2014; 63: 1123–1133. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
