

A multigenomic liquid biopsy biomarker for neuroendocrine tumor disease outperforms CgA and has surgical and clinical utility
- PMID: 34390828
- PMCID: PMC9393904
- DOI: 10.1016/j.annonc.2021.08.1746
A multigenomic liquid biopsy biomarker for neuroendocrine tumor disease outperforms CgA and has surgical and clinical utility
Abstract
Background: Biomarkers are key tools in cancer management. In neuroendocrine tumors (NETs), Chromogranin A (CgA) was considered acceptable as a biomarker. We compared the clinical efficacy of a multigenomic blood biomarker (NETest) to CgA over a 5-year period.
Patients and methods: An observational, prospective, cross-sectional, multicenter, multinational, comparative cohort assessment. Cohort 1: NETest evaluation in NETs (n = 1684) and cancers, benign diseases, controls (n = 731). Cohort 2: (n = 1270): matched analysis of NETest/CgA in a sub-cohort of NETs (n = 922) versus other diseases and controls (n = 348). Disease status was assessed by response evaluation criteria in solid tumors (RECIST). NETest measurement: qPCR [upper limit of normal (ULN: 20)], CgA (EuroDiagnostica, ULN: 108 ng/ml).
Statistics: Mann-Whitney U-test, AUROC, chi-square and McNemar' test.
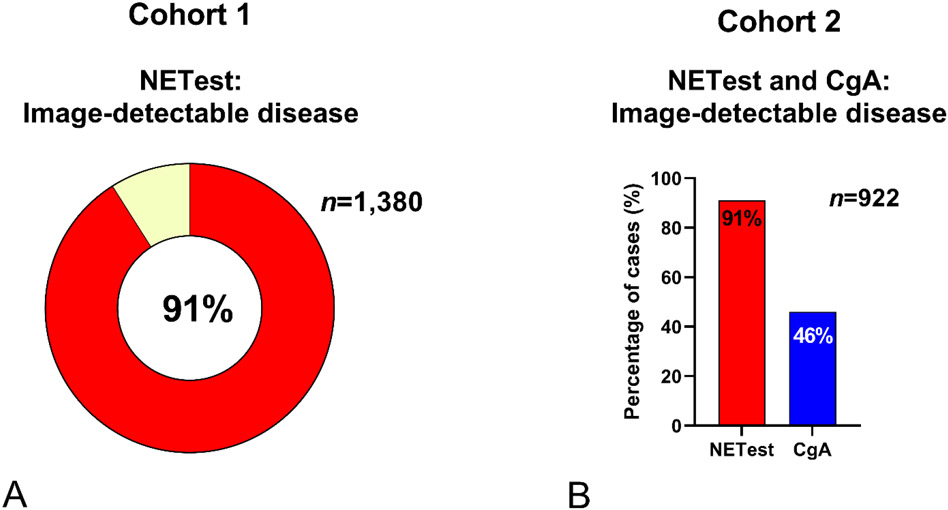
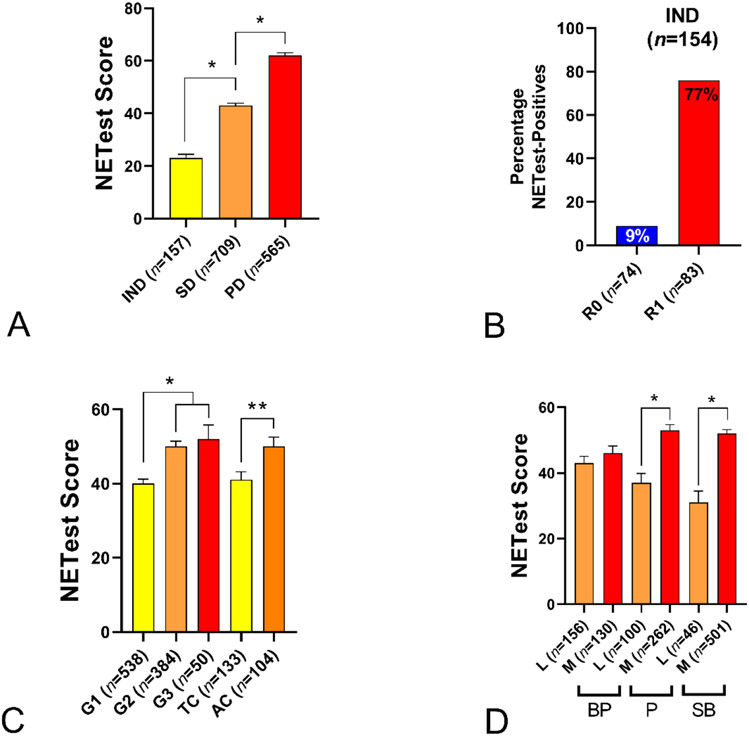
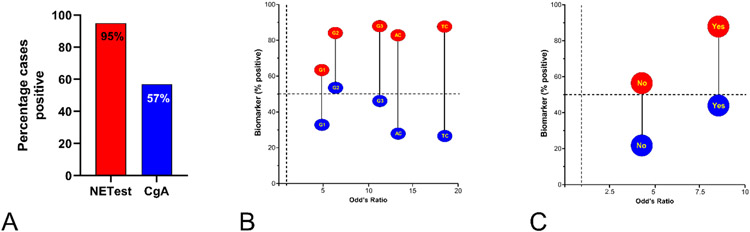
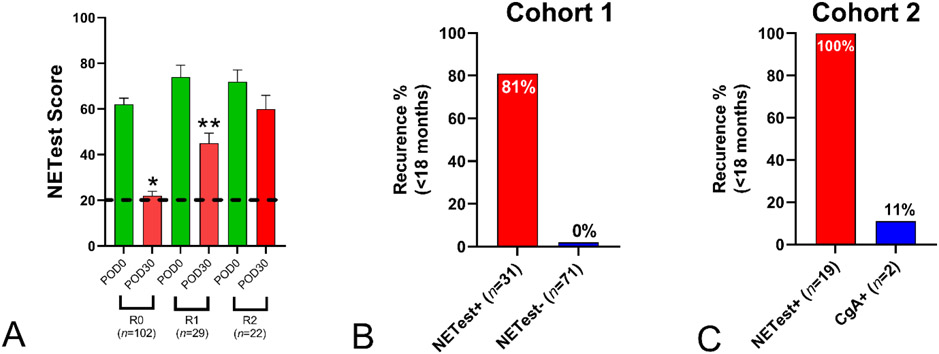
Results: Cohort 1: NETest diagnostic accuracy was 91% (P < 0.0001) and identified pheochromocytomas (98%), small intestine (94%), pancreas (91%), lung (88%), gastric (80%) and appendix (79%). NETest reflected grading: G1: 40 ± 1, G2 (50 ± 1) and G3 (52 ± 1). Locoregional disease levels were lower (38 ± 1) than metastatic (52 ± 1, P < 0.0001). NETest accurately stratified RECIST-assessed disease extent: no disease (21 ± 1), stable (43 ± 2), progressive (62 ± 2) (P < 0.0001). NETest concordance with imaging (CT/MRI/68Ga-SSA-PET) 91%. Presurgery, all NETs (n = 153) were positive (100%). After palliative R1/R2 surgery (n = 51) all (100%) remained elevated. After curative R0-surgery (n = 102), NETest levels were normal in 81 (70%) with no recurrence at 2 years. In the 31 (30%) with elevated levels, 25 (81%) recurred within 2 years. Cohort #2: NETest diagnostic accuracy was 87% and CgA 54% (P < 0.0001). NETest was more accurate than CgA for grading (chi-square = 7.7, OR = 18.5) and metastatic identification (chi-square = 180, OR = 8.4). NETest identified progressive disease (95%) versus CgA (57%, P < 0.0001). Imaging concordance for NETest was 91% versus CgA (46%) (P < 0.0001). Recurrence prediction after surgery was NETest-positive in >94% versus CgA 11%.
Conclusion: NETest accurately diagnoses NETs and is an effective surrogate marker for imaging, grade, metastases and disease status compared to CgA. A multigenomic liquid biopsy is an accurate biomarker of NET disease.
Keywords: Chromogranin; NET; NETest; biomarker; neuroendocrine tumor.
Copyright © 2021 European Society for Medical Oncology. All rights reserved.
Conflict of interest statement
Disclosure KEÖ is a senior professor Uppsala University, has received honoraria from Novartis, IPSEN, AAA, DQS, Wren, Camurus and ITM. Centers of Excellence reviewer for ENETS. IMM: consultant for Novartis, Ipsen, Wren, Wyeth, Nycomed, RadioMedix and Mallinckrodt. MK: employee of Wren. MF: research grants and advisory role for: J&J, Novartis, Ipsen, AAA, Mylan and Celgene. AF: has received educational grants and research grants from Novartis. Speaker honorarium from Novartis for work not related to the present paper. CT: IPSEN honoraria for lectures, advisory boards and educational grants. LB: unpaid consultant/advisor AAA and Ipsen. All other authors have declared no conflicts of interest.
Figures

References
-
- Perera FP, Weinstein IB. Molecular epidemiology: recent advances and future directions. Carcinogenesis 2000; 21: 517–524. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
