

Posterior pericardiotomy to prevent new-onset atrial fibrillation after coronary artery bypass grafting: a systematic review and meta-analysis of 10 randomized controlled trials
- PMID: 34391454
- PMCID: PMC8364072
- DOI: 10.1186/s13019-021-01611-x
Posterior pericardiotomy to prevent new-onset atrial fibrillation after coronary artery bypass grafting: a systematic review and meta-analysis of 10 randomized controlled trials
Abstract
Background: Atrial fibrillation (AF) is associated with adverse events after cardiac surgery. Multiple studies have reported that posterior pericardiotomy (PP) may be effective for preventing AF after coronary artery bypass grafting (CABG), but some conflicting results have been reported and the quality of evidence from previous meta-analyses has been limited. The present study aimed to systematically evaluate the safety and efficacy of PP for preventing AF after CABG in adults.
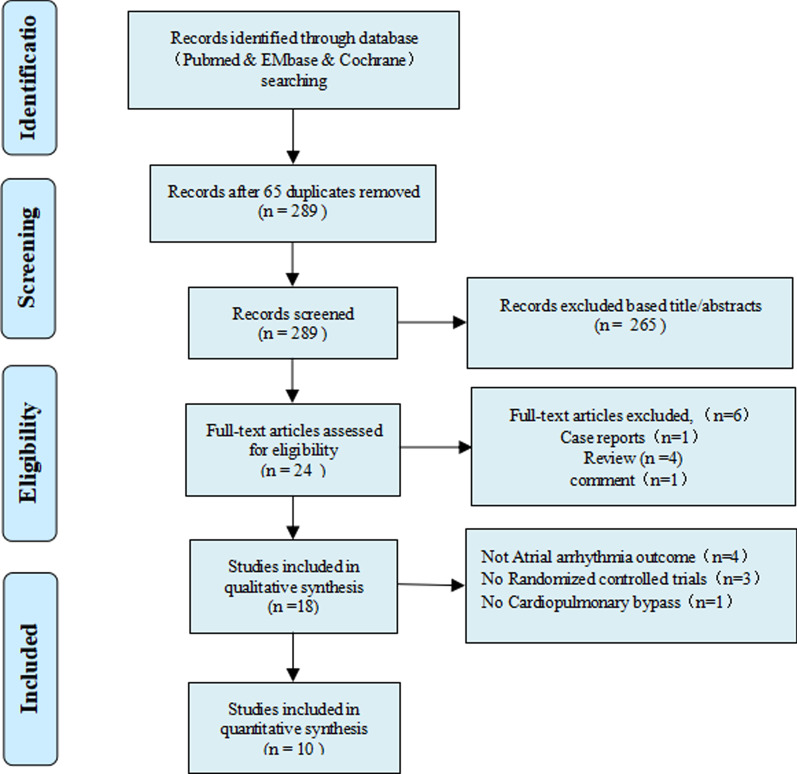
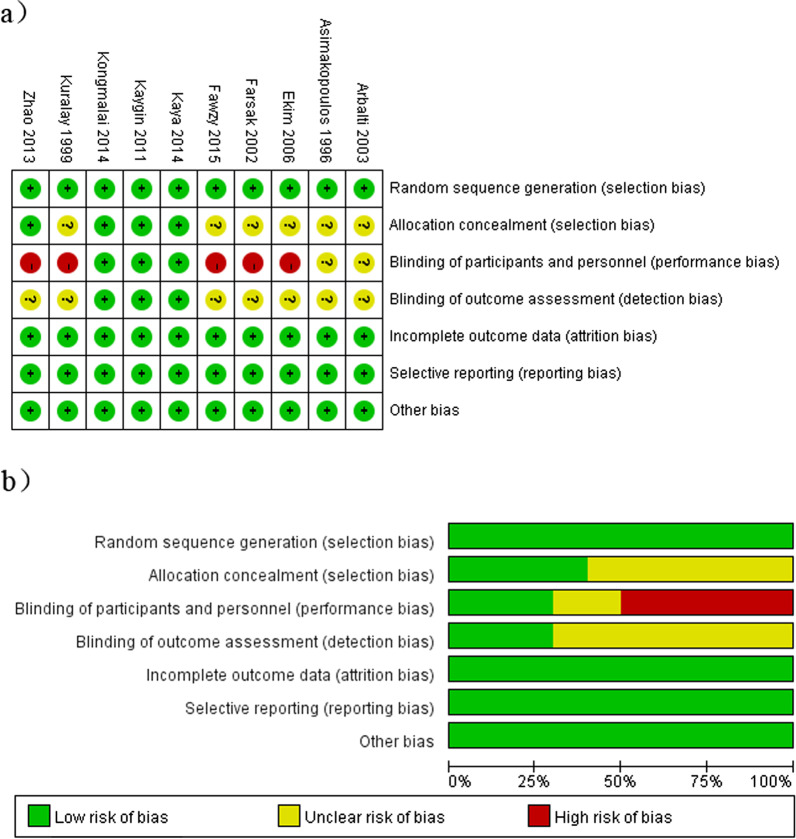
Methods: We conducted a quantitative meta-analysis of randomized controlled trials (RCTs) published before May 31, 2021. The primary outcome was AF after CABG under cardiopulmonary bypass. Secondary outcomes included early pericardial effusion, late pericardial effusion, pericardial tamponade, pleural effusion, length of hospital stay, length of intensive care unit (ICU) stay, pulmonary complications, intra-aortic balloon pump use, revision surgery for bleeding, and mortality.
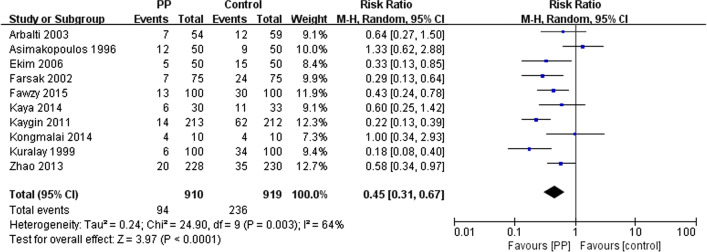
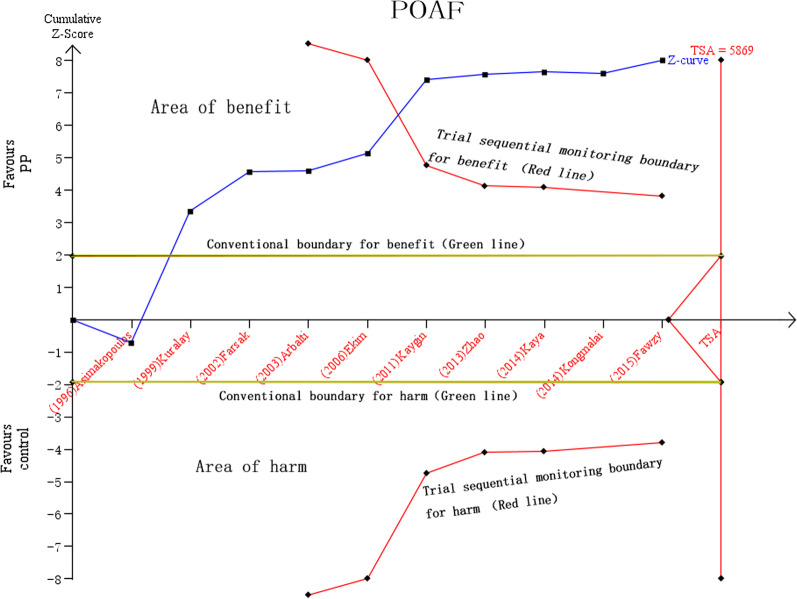
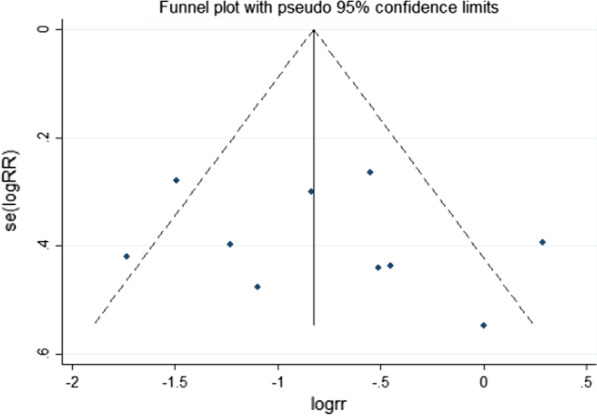
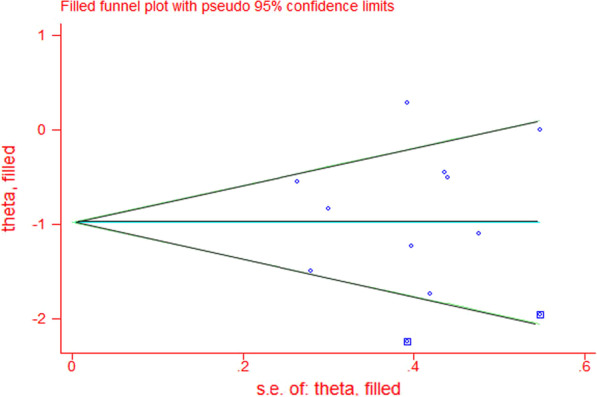
Results: Ten RCTs with 1829 patients (910 in the PP group and 919 in the control group) were included in the current meta-analysis. The incidence of AF was 10.3% (94/910) in the PP group and 25.7% (236/919) in the control group. A random-effects model indicated that incidence of AF after CABG significantly lower in the PP group than in the control group (risk ratio = 0.45, 95% confidence interval 0.29-0.64, P < 0.0001). PP also effectively reduced the post-CABG occurrence of early pericardial effusion (RR = 0.28, 95% CI 0.15-0.50; P < 0.05), late pericardial effusion (RR = 0.06, 95% CI 0.02-0.16; P < 0.05), and pericardial tamponade (RR = 0.08, 95% CI 0.02-0.33; P < 0.05) as well as the length of ICU stay (weighted mean difference [WMD] = 0.91,95% CI 0.57-1.24; P < 0.05), while increasing the occurrence pleural effusion (RR = 1.51, 95% CI 1.19-1.92; P < 0.05). No significant differences length of hospital stay (WMD = - 0.45, 95% CI - 2.44 to 1.54, P = 0.66), pulmonary complications (RR = 0.99, 95% CI 0.71-1.39, P = 0.97), revision surgery for bleeding (RR = 0.84, 95% CI 0.43-1.63, P = 0.60), use of IABP (RR = 1, 95% CI 0.61-1.65, P = 1.0), or death (RR = 0.45, 95% CI 0.07-3.03, P = 0.41) were observed between the PP and control groups.
Conclusions: PP may be a safe, effective, and economical method for preventing AF after CABG in adult patients.
Keywords: Coronary artery bypass grafting; Posterior pericardiotomy; Postoperative atrial fibrillation.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no conflicts of interest with this research.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
