A radiological predictor for pneumomediastinum/pneumothorax in COVID-19 ARDS patients
- PMID: 34392131
- PMCID: PMC8357628
- DOI: 10.1016/j.jcrc.2021.07.022
A radiological predictor for pneumomediastinum/pneumothorax in COVID-19 ARDS patients
Abstract
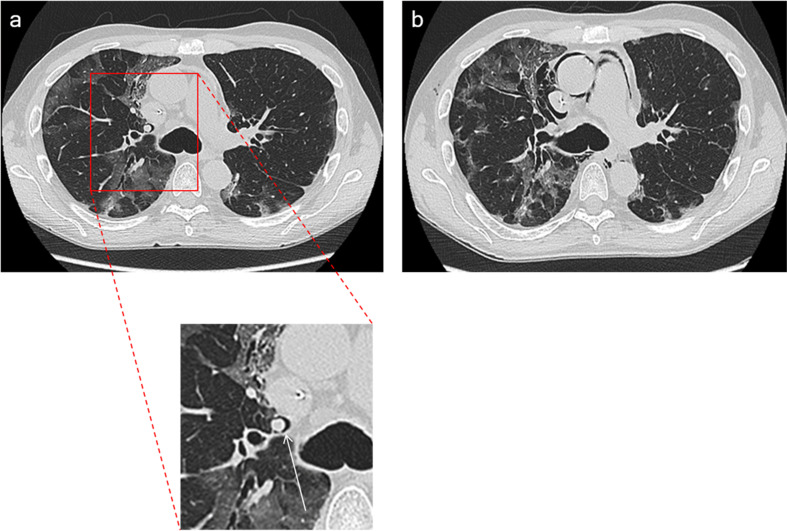
Purpose: To determine whether Macklin effect (a linear collection of air contiguous to the bronchovascular sheath) on baseline CT imaging is an accurate predictor for subsequent pneumomediastinum (PMD)/pneumothorax (PNX) development in invasively ventilated patients with COVID-19-related acute respiratory distress syndrome (ARDS).
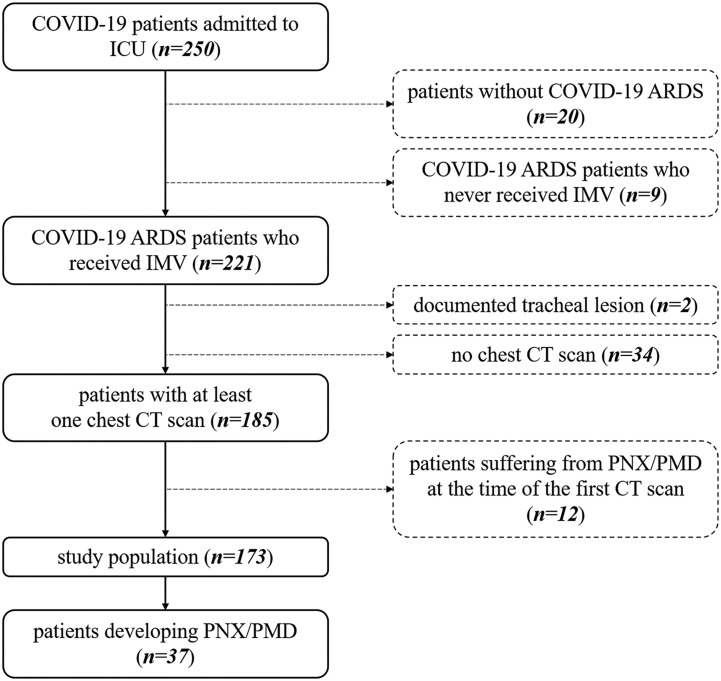
Materials and methods: This is an observational, case-control study. From a prospectively acquired database, all consecutive invasively ventilated COVID-19 ARDS patients who underwent at least one baseline chest CT scan during the study time period (February 25th, 2020-December 31st, 2020) were identified; those who had tracheal lesion or already had PMD/PNX at the time of the first available chest imaging were excluded.
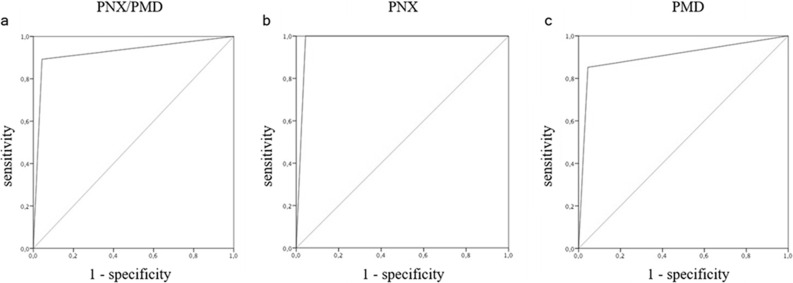
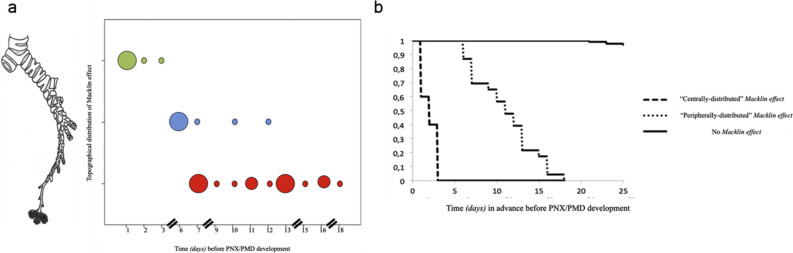
Results: 37/173 (21.4%) patients enrolled had PMD/PNX; specifically, 20 (11.5%) had PMD, 10 (5.8%) PNX, 7 (4%) both. 33/37 patients with subsequent PMD/PNX had Macklin effect on baseline CT (89.2%, true positives) 8.5 days [range, 1-18] before the first actual radiological evidence of PMD/PNX. Conversely, 6/136 patients without PMD/PNX (4.4%, false positives) demonstrated Macklin effect (p < 0.001). Macklin effect yielded a sensitivity of 89.2% (95% confidence interval [CI]: 74.6-96.9), a specificity of 95.6% (95% CI: 90.6-98.4), a positive predictive value (PV) of 84.5% (95% CI: 71.3-92.3), a negative PV of 97.1% (95% CI: 74.6-96.9) and an accuracy of 94.2% (95% CI: 89.6-97.2) in predicting PMD/PNX (AUC:0.924).
Conclusions: Macklin effect accurately predicts, 8.5 days in advance, PMD/PNX development in COVID-19 ARDS patients.
Keywords: Acute respiratory distress syndrome; COVID-19; Mechanical ventilation; Pneumomediastinum; Pneumothorax; Tomography, X-ray computed.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest None.
Figures