

ESR1 mutation as an emerging clinical biomarker in metastatic hormone receptor-positive breast cancer
- PMID: 34392831
- PMCID: PMC8365900
- DOI: 10.1186/s13058-021-01462-3
ESR1 mutation as an emerging clinical biomarker in metastatic hormone receptor-positive breast cancer
Abstract
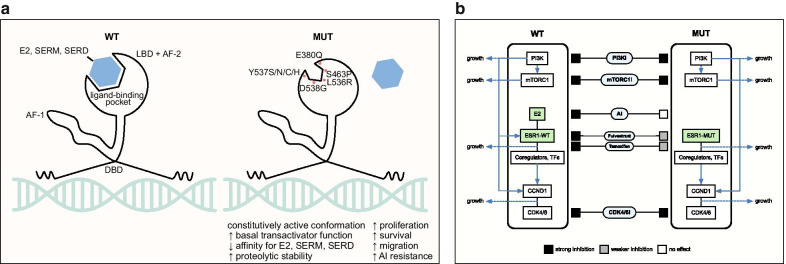
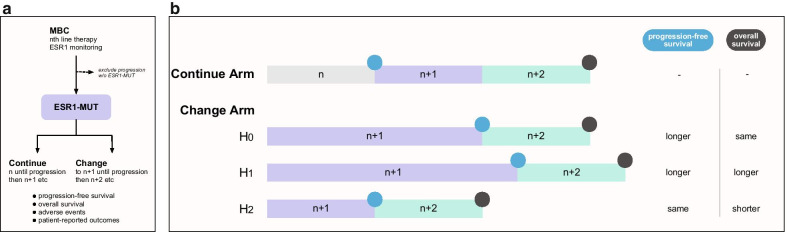
In metastatic hormone receptor-positive breast cancer, ESR1 mutations are a common cause of acquired resistance to the backbone of therapy, estrogen deprivation by aromatase inhibition. How these mutations affect tumor sensitivity to established and novel therapies are active areas of research. These therapies include estrogen receptor-targeting agents, such as selective estrogen receptor modulators, covalent antagonists, and degraders (including tamoxifen, fulvestrant, and novel agents), and combination therapies, such as endocrine therapy plus CDK4/6, PI3K, or mTORC1 inhibition. In this review, we summarize existing knowledge surrounding the mechanisms of action of ESR1 mutations and roles in resistance to aromatase inhibition. We then analyze the recent literature on how ESR1 mutations affect outcomes in estrogen receptor-targeting and combination therapies. For estrogen receptor-targeting therapies such as tamoxifen and fulvestrant, ESR1 mutations cause relative resistance in vitro but do not clearly lead to resistance in patients, making novel agents in this category promising. Regarding combination therapies, ESR1 mutations nullify any aromatase inhibitor component of the combination. Thus, combinations using endocrine alternatives to aromatase inhibition, or combinations where the non-endocrine component is efficacious as monotherapy, are still effective against ESR1 mutations. These results emphasize the importance of investigating combinatorial resistance, challenging as these efforts are. We also discuss future directions and open questions, such as studying the differences among distinct ESR1 mutations, asking how to adjust clinical decisions based on molecular surveillance testing, and developing novel therapies that are effective against ESR1 mutations.
Keywords: Breast cancer; CDK4/6; Combination; ESR1 mutation; Hormone receptor/estrogen receptor; Resistance; SERCA; SERD; SERM.
© 2021. The Author(s).
Conflict of interest statement
AB reports consulting/advisory board fees from Pfizer, Novartis, Genentech, Merck, Radius Health, Immunomedics, Taiho, Sanofi, Daiichi Pharma/Astra Zeneca, Puma Biotechnology, Biothernostics Inc., Phillips, Eli Lilly, and Foundation Medicine, and contracted research/grants (to institution) from Genentech, Novartis, Pfizer, Merck, Sanofi, Radius Health, Immunomedics, and Daiichi Pharma/Astra Zeneca. LMS reports consulting/advisory board fees from Novartis and Avrobio. SAW reports consulting fees from Foundation Medicine and Veracyte as well as institutional funding from Genentech.
Figures
References
-
- Zhang QX, Borg A, Wolf DM, Oesterreich S, Fuqua SA. An estrogen receptor mutant with strong hormone-independent activity from a metastatic breast cancer. Cancer Res. 1997;57:1244–1249. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
