

Safety and efficacy of thromboelastography guidance of antifibrinolytic therapy in trauma patients: An observational cohort analysis
- PMID: 34395207
- PMCID: PMC8318174
- DOI: 10.4103/IJCIIS.IJCIIS_79_20
Safety and efficacy of thromboelastography guidance of antifibrinolytic therapy in trauma patients: An observational cohort analysis
Abstract
Background: Tranexamic acid (TXA) is an antifibrinolytic therapy intended to decrease blood loss and improve hemostasis in traumatic hemorrhage. Viscoelastic assays, such as thromboelastography (TEG), allow for the identification of a patient's specific hemostasis. The purpose of this research study was to explore the safety and efficacy of TEG-guided antifibrinolytic therapy in trauma patients.
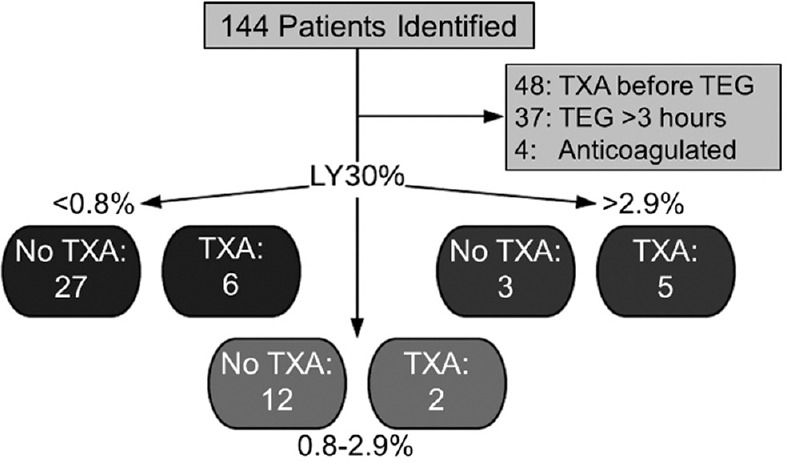
Methods: This study was a retrospective review of trauma patients meeting institution-specific inclusion criteria for TXA. Patients were assigned to fibrinolytic groups per TEG LY30 data. Safety outcomes (24-h mortality, overall in-hospital mortality, and thromboembolic events) were compared between patients who did or did not receive TXA and within fibrinolytic groups. Mortality outcomes were adjusted for baseline Injury Severity Score (ISS). Secondary aims included blood product utilization, length of hospital, and intensive care unit stay.
Results: Hypofibrinolysis was the most common fibrinolytic phenotype. Adjusting for ISS, there were no significant differences in mortality. A 30.7% thromboembolism incidence was identified in the TXA group compared to 16.6% not receiving TXA (P = 0.26), with 72.7% of these patients experiencing fibrinolytic shutdown.
Conclusions: There were no differences in 24-h mortality, all-cause mortality, or secondary outcomes. The difference in thromboembolic rates between patients receiving TXA and those who did not, while not statistically significant, poses clinical concern.
Keywords: Antifibrinolytic agents; Injury Severity Score; thromboelastography; tranexamic acid; wounds and injuries.
Copyright: © 2021 International Journal of Critical Illness and Injury Science.
Conflict of interest statement
There are no conflicts of interest.
Figures



References
-
- Huang F, Wu D, Ma G, Yin Z, Wang Q. The use of tranexamic acid to reduce blood loss and transfusion in major orthopedic surgery: A meta-analysis. J Surg Res. 2014;186:318–27. - PubMed
-
- Shakur H, Roberts I, Bautista R, Caballero J, Coats T, Dewan Y, et al. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant hemorrhage (CRASH-2): A randomized, placebo-controlled trial. Lancet. 2010;376:23–32. - PubMed
-
- Bolliger D, Seeberger MD, Tanaka KA. Principles and practice of thromboelastography in clinical coagulation management and transfusion practice. Transfus Med Rev. 2012;26:1–13. - PubMed
-
- Abdelfattah K, Cripps MW. Thromboelastography and rotational thromboelastometry use in trauma. Int J Surg. 2016;33:196–201. - PubMed
LinkOut - more resources
Full Text Sources