

Ischemia and Bleeding in Cancer Patients Undergoing Percutaneous Coronary Intervention
- PMID: 34396175
- PMCID: PMC8352169
- DOI: 10.1016/j.jaccao.2019.11.001
Ischemia and Bleeding in Cancer Patients Undergoing Percutaneous Coronary Intervention
Abstract
Objectives: The purpose of this study was to evaluate ischemic and bleeding outcomes of unselected cancer patients undergoing percutaneous coronary intervention (PCI).
Background: The number of cancer patients undergoing PCI is increasing despite concerns regarding ischemic and bleeding risks.
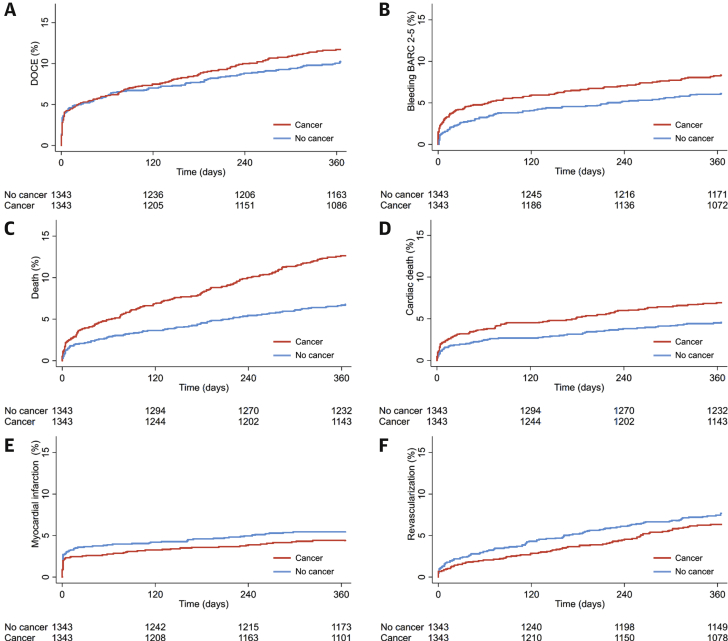
Methods: Between 2009 and 2017, consecutive patients undergoing PCI were prospectively included in the Bern PCI Registry. Cancer-specific data including type, date of initial diagnosis, and health status at index PCI were collected. We performed propensity score matching to adjust for baseline differences between patients with and without cancer. The primary ischemic endpoint was the device-oriented composite endpoint (cardiac death, target vessel myocardial infarction, target lesion revascularization) at 1 year, and the primary bleeding endpoint was Bleeding Academic Research Consortium (BARC) 2 to 5 at 1 year.
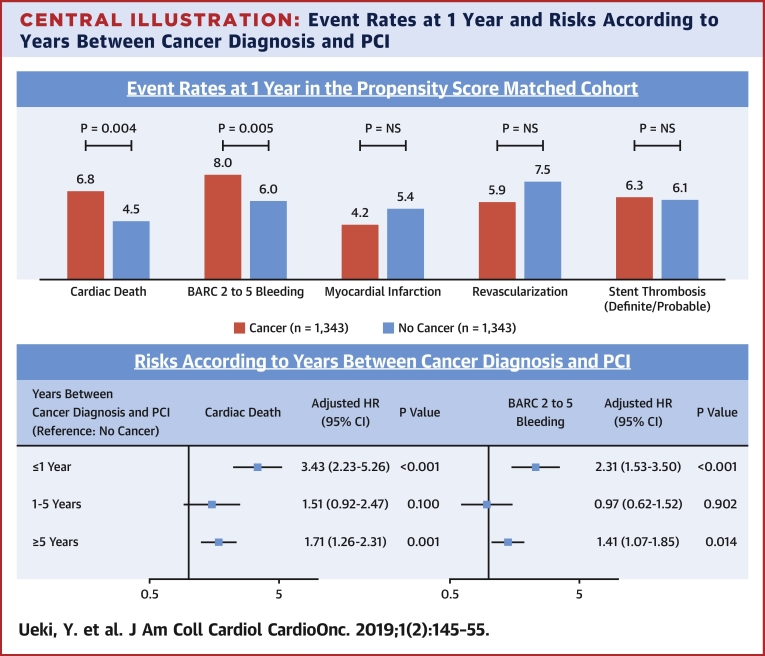
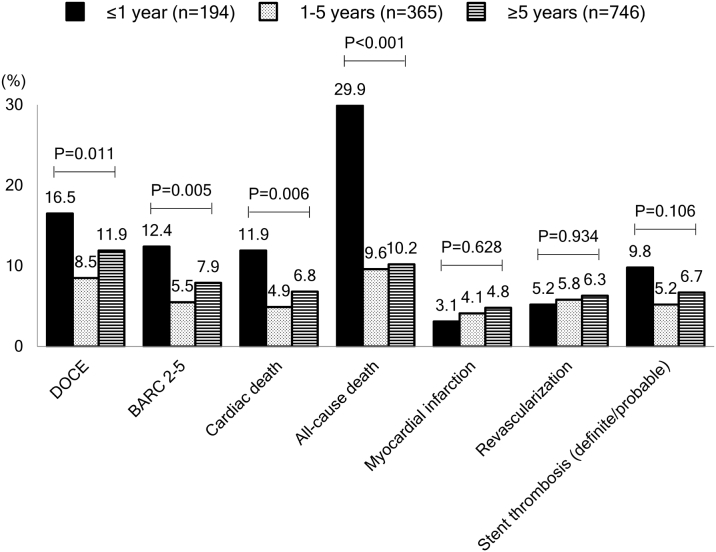
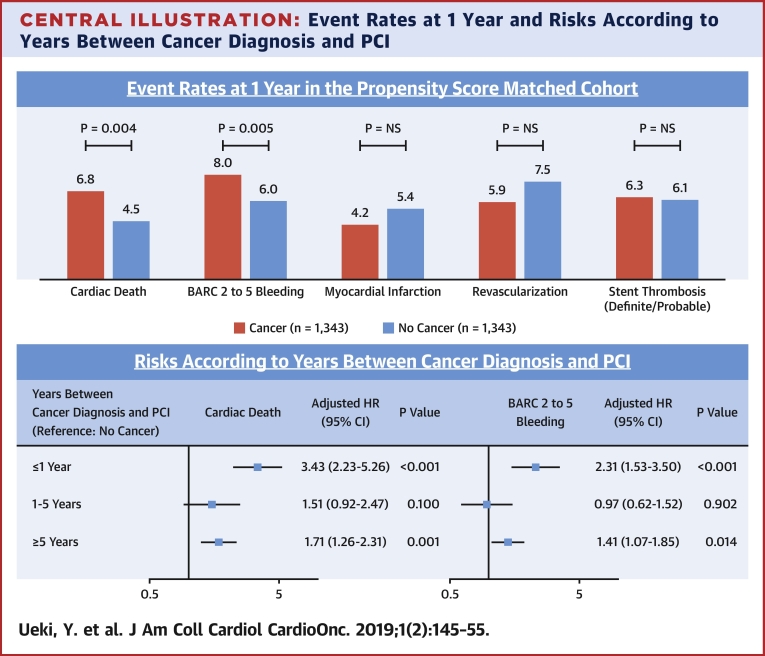
Results: Among 13,647 patients, 1,368 (10.0%) had an established diagnosis of cancer. The 3 leading cancer types were prostate (n = 294), gastrointestinal tract (n = 188), and hematopoietic (n = 177). At index PCI, 179 (13.1%) patients were receiving active cancer treatment. In matched analysis, there was no significant difference in device-oriented composite endpoint (11.5% vs. 10.2%; p = 0.251), whereas cardiac death and BARC 2 to 5 bleeding occurred more frequently among patients with cancer compared with those without cancer (6.8% vs. 4.5%; p = 0.010 and 8.0% vs. 6.0%; p = 0.026, respectively). Cancer diagnosis within 1 year before PCI emerged as an independent predictor for cardiac death and BARC 2 to 5 bleeding at 1 year.
Conclusions: Cancer patients carry an increased risk of cardiac mortality that was not associated with stent-related ischemic events among patients undergoing PCI in routine clinical practice. Higher risk of bleeding in cancer patients undergoing PCI deserves particular attention. (CARDIOBASE Bern PCI Registry; NCT02241291).
Keywords: BARC, Bleeding Academic Research Consortium; CAD, coronary artery disease; CI, confidence interval; DAPT, dual antiplatelet therapy; DES, drug-eluting stent; DOCE, device-oriented composite endpoint; HR, hazard ratio; IPTW, inverse probability of treatment weighting; MI, myocardial infarction; PCI, percutaneous coronary interventions; PS, propensity score; bleeding; cancer; coronary artery disease; ischemia; percutaneous coronary intervention.
© 2019 The Authors.
Figures
References
-
- Rickles F.R. Mechanisms of cancer-induced thrombosis in cancer. Pathophysiol Haemost Thromb. 2006;35:103–110. - PubMed
-
- Darby S.C., Ewertz M., McGale P. Risk of ischemic heart disease in women after radiotherapy for breast cancer. N Engl J Med. 2013;368:987–998. - PubMed
-
- Frickhofen N., Beck F.J., Jung B., Fuhr H.G., Andrasch H., Sigmund M. Capecitabine can induce acute coronary syndrome similar to 5-fluorouracil. Ann Oncol. 2002;13:797–801. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
