

Reduced Cardiorespiratory Fitness and Increased Cardiovascular Mortality After Prolonged Androgen Deprivation Therapy for Prostate Cancer
- PMID: 34396266
- PMCID: PMC8352085
- DOI: 10.1016/j.jaccao.2020.08.011
Reduced Cardiorespiratory Fitness and Increased Cardiovascular Mortality After Prolonged Androgen Deprivation Therapy for Prostate Cancer
Abstract
Background: Prolonged androgen deprivation therapy (ADT) is favored over short-term use in patients with localized high-risk prostate cancer (PC).
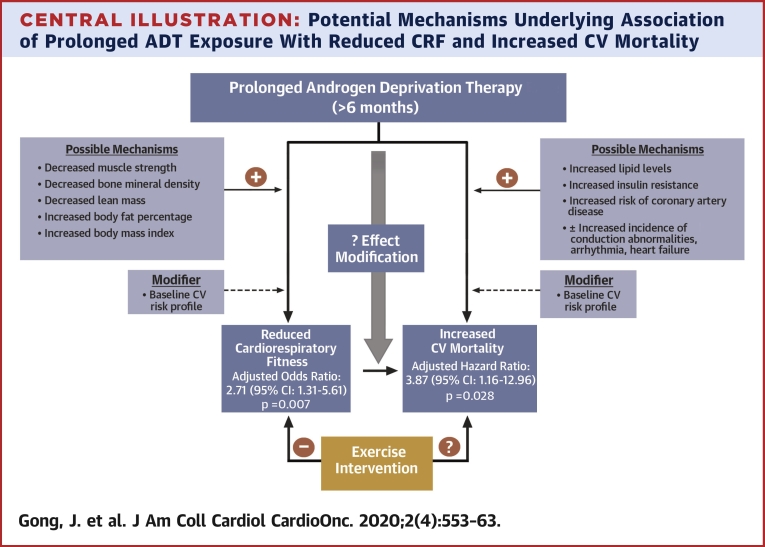
Objectives: This study sought to compare cardiorespiratory fitness (CRF) and cardiovascular (CV) mortality among patients with PC with and without ADT exposure and to explore how duration of ADT exposure influences CRF and CV mortality.
Methods: Retrospective cohort study of patients referred for exercise treadmill testing (ETT) after a PC diagnosis. PC risk classification was based on Gleason score (GS): high risk if GS ≥8; intermediate risk if GS = 7; and low risk if GS <7. CRF was categorized by metabolic equivalents (METs): METs >8 defined as good CRF and METs ≤8 as reduced CRF. ADT exposure was categorized as short term (≤6 months) versus prolonged (>6 months).
Results: A total of 616 patients underwent an ETT a median of 4.8 years (interquartile range: 2.0, 7.9 years) after PC diagnosis. Of those, 150 patients (24.3%) received ADT prior to the ETT; 99 with short-term and 51 with prolonged exposure. 504 patients (81.8%) had ≥2 CV risk factors. Prolonged ADT was associated with reduced CRF (odds ratio [OR]: 2.71; 95% confidence interval [CI]: 1.31 to 5.61; p = 0.007) and increased CV mortality (hazard ratio [HR]: 3.87; 95% CI: 1.16 to 12.96; p = 0.028) in adjusted analyses. Although the association between short-term ADT exposure and reduced CRF was of borderline significance (OR: 1.71; 95% CI: 1.00 to 2.94; p = 0.052), there was no association with CV mortality (HR: 1.60; 95% CI: 0.51 to 5.01; p = 0.420) in adjusted Cox regression models.
Conclusions: Among patients with PC and high baseline CV risk, prolonged ADT exposure was associated with reduced CRF and increased CV mortality.
Keywords: ADT, androgen deprivation therapy; BMI, body mass index; CI, confidence interval; CRF, cardiorespiratory fitness; CV, cardiovascular; ETT, exercise treadmill test; HR, hazard ratio; IQR, interquartile range; MET, metabolic equivalent; OR, odds ratio; PC, prostate cancer; androgen deprivation therapy; cardio-oncology; cardiorespiratory fitness; cardiovascular mortality; cardiovascular risk; prostate cancer.
© 2020 The Authors.
Conflict of interest statement
This work was supported by the Goodman Master Clinician Award from Brigham and Women’s Hospital (to Dr. Groarke) and by the Gelb Master Clinician Award and the Catherine Fitch Fund form Brigham and Women’s Hospital (to Dr. Nohria). Dr. McGregor has served as a consultant for Bayer, Astellas, AstraZeneca, Seattle Genetics, Exelixis, Nektar, Pfizer, Janssen, and Genentech; and has received research support paid to his institution from Bristol Myers Squibb. Dr. Neilan was supported in part through a gift from A. Curt Greer, Pamela Greer, and Kohlberg Foundation, National Institutes of Health/National Heart, Lung, and Blood Institute (grants 1R01HL130539-01A1, 1R01HL137562-01A1, K24HL113128-06), and National Institutes of Health/Harvard Center for AIDS Research (grant P30 AI060354). Dr. Nohria has served as a consultant for Takeda Oncology and Triple Gene Therapy; and has received research support from Amgen, Inc. Dr. Groarke has received research support from Amgen, Inc. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures




References
-
- American Cancer Society . American Cancer Society; Atlanta, GA: 2014. Cancer Treatment and Survivorship Facts and Figures 2014–2015.
-
- Meng M.V., Grossfeld G.D., Sadetsky N., Mehta S.S., Lubeck D.P., Carroll P.R. Contemporary patterns of androgen deprivation therapy use for newly diagnosed prostate cancer. Urology. 2002;60(Suppl 1):7–11. discussion 11–2. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
