

Refining the 10-Year Prediction of Left Ventricular Systolic Dysfunction in Long-Term Survivors of Childhood Cancer
- PMID: 34396306
- PMCID: PMC8352242
- DOI: 10.1016/j.jaccao.2020.11.013
Refining the 10-Year Prediction of Left Ventricular Systolic Dysfunction in Long-Term Survivors of Childhood Cancer
Abstract
Background: In childhood cancer survivors (CCS) at risk for heart failure, echocardiographic surveillance recommendations are currently based on anthracyclines and chest-directed radiotherapy dose. Whether the ejection fraction (EF) measured at an initial surveillance echocardiogram can refine these recommendations is unknown.
Objectives: The purpose of this study was to assess the added predictive value of EF at >5 years after cancer diagnosis to anthracyclines and chest-directed radiotherapy dose in CCS, for the development of left ventricular dysfunction with an ejection fraction <40% (LVD40).
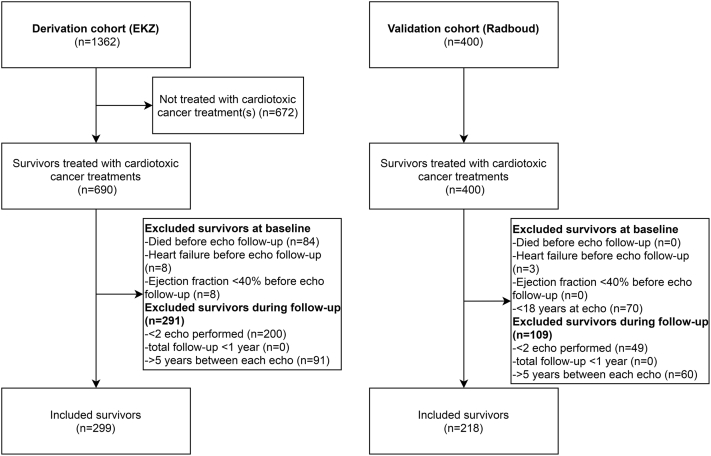
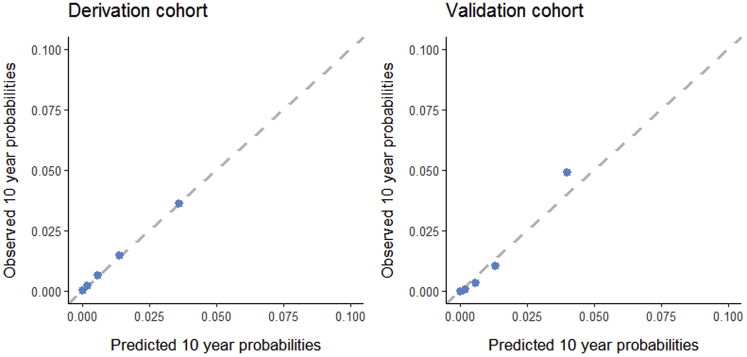
Methods: Echocardiographic surveillance was performed in 299 CCS from the Emma Children's Hospital in the Netherlands. Cox regression models were built including cardiotoxic cancer treatment exposures with and without EF to estimate the probability of LVD40 at 10-year follow-up. Calibration, discrimination, and reclassification were assessed. Results were externally validated in 218 CCS.
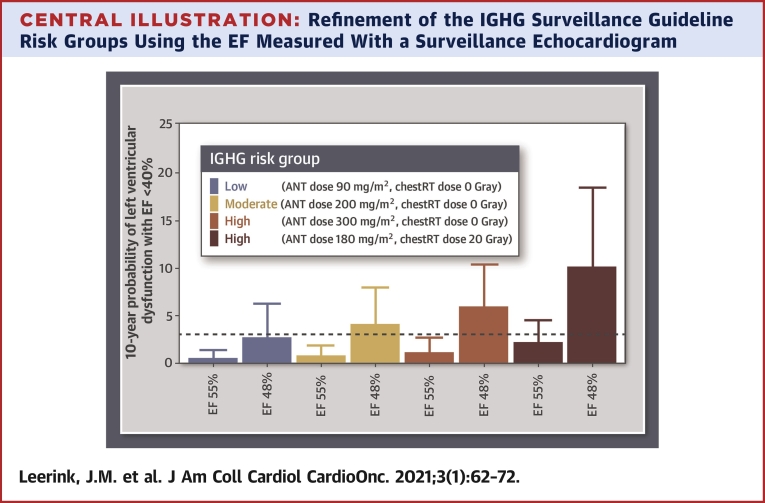
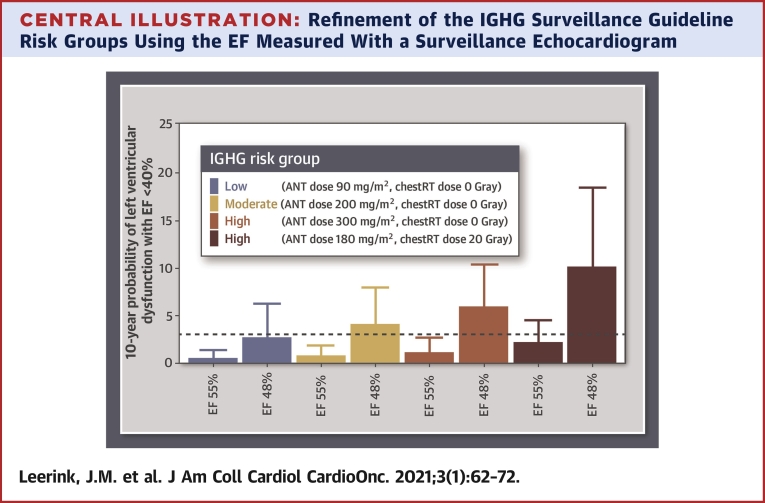
Results: Cumulative incidences of LVD40 at 10-year follow-up were 3.7% and 3.6% in the derivation and validation cohort, respectively. The addition of EF resulted in an integrated area under the curve increase from 0.74 to 0.87 in the derivation cohort and from 0.72 to 0.86 in the validation cohort (likelihood ratio p < 0.001). Reclassification of CCS without LVD40 improved significantly (noncase continuous net reclassification improvement 0.50; 95% confidence interval [CI]: 0.40 to 0.60). A predicted LVD40 probability ≤3%, representing 75% of the CCS, had a negative predictive value of 99% (95% CI: 98% to 100%) for LVD40 within 10 years. However, patients with midrange EF (40% to 49%) at initial screening had an incidence of LVD40 of 11% and a 7.81-fold (95% CI: 2.07- to 29.50-fold) increased risk of LV40 at follow-up.
Conclusions: In CCS, an initial surveillance EF, in addition to anthracyclines and chest-directed radiotherapy dose, improves the 10-year prediction for LVD40. Through this strategy, both the identification of low-risk survivors in whom the surveillance frequency may be reduced and a group of survivors at increased risk of LVD40 could be identified.
Keywords: CCS, childhood cancer survivors; CI, confidence interval; EF, ejection fraction; LVD40, left ventricular dysfunction with an ejection fraction <40%; cardio-oncology; childhood cancer survivors; echocardiography; risk prediction model; surveillance.
© 2021 The Authors.
Conflict of interest statement
This study was funded by a Dutch Heart Foundation Grant (CVON2015-21). The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Similar articles
-
Extensive Cardiac Function Analyses Using Contemporary Echocardiography in Childhood Cancer Survivors: A DCCSS LATER Study.JACC CardioOncol. 2023 Aug 15;5(4):472-485. doi: 10.1016/j.jaccao.2023.06.003. eCollection 2023 Aug. JACC CardioOncol. 2023. PMID: 37614574 Free PMC article.
-
Cardiac Events in Childhood Cancer Survivors Treated with Anthracyclines: The Value of Previous Myocardial Strain Measurement.Life (Basel). 2022 Mar 19;12(3):452. doi: 10.3390/life12030452. Life (Basel). 2022. PMID: 35330203 Free PMC article.
-
Valvular abnormalities detected by echocardiography in 5-year survivors of childhood cancer: a long-term follow-up study.Int J Radiat Oncol Biol Phys. 2015 Jan 1;91(1):213-22. doi: 10.1016/j.ijrobp.2014.09.010. Epub 2014 Oct 25. Int J Radiat Oncol Biol Phys. 2015. PMID: 25442333
-
Educational paper: decreasing the burden of cardiovascular disease in childhood cancer survivors: an update for the pediatrician.Eur J Pediatr. 2013 Sep;172(9):1149-60. doi: 10.1007/s00431-013-1931-9. Epub 2013 Jan 30. Eur J Pediatr. 2013. PMID: 23361962 Review.
-
Cardiac Disease in Childhood Cancer Survivors: Risk Prediction, Prevention, and Surveillance: JACC CardioOncology State-of-the-Art Review.JACC CardioOncol. 2020 Sep 15;2(3):363-378. doi: 10.1016/j.jaccao.2020.08.006. eCollection 2020 Sep. JACC CardioOncol. 2020. PMID: 34396245 Free PMC article. Review.
Cited by
-
Automated Global Longitudinal Strain Assessment in Long-Term Survivors of Childhood Acute Lymphoblastic Leukemia.Cancers (Basel). 2022 Mar 15;14(6):1513. doi: 10.3390/cancers14061513. Cancers (Basel). 2022. PMID: 35326663 Free PMC article.
-
Rurality, Cardiovascular Risk Factors, and Early Cardiovascular Disease among Childhood, Adolescent, and Young Adult Cancer Survivors.Res Sq [Preprint]. 2024 Apr 1:rs.3.rs-4139837. doi: 10.21203/rs.3.rs-4139837/v1. Res Sq. 2024. Update in: J Adolesc Young Adult Oncol. 2025 Mar 25. doi: 10.1089/jayao.2024.0151. PMID: 38645102 Free PMC article. Updated. Preprint.
-
Improved Cardiomyopathy Risk Prediction Using Global Longitudinal Strain and N-Terminal-Pro-B-Type Natriuretic Peptide in Survivors of Childhood Cancer Exposed to Cardiotoxic Therapy.J Clin Oncol. 2024 Apr 10;42(11):1265-1277. doi: 10.1200/JCO.23.01796. Epub 2024 Jan 11. J Clin Oncol. 2024. PMID: 38207238 Free PMC article.
-
Obesity Predisposes Anthracycline-Treated Survivors of Childhood and Adolescent Cancers to Subclinical Cardiac Dysfunction.Pediatr Cardiol. 2025 Feb;46(2):362-371. doi: 10.1007/s00246-024-03423-x. Epub 2024 Mar 8. Pediatr Cardiol. 2025. PMID: 38456890
-
The burden of cardiovascular disease and risk for subsequent major adverse cardiovascular events in survivors of childhood cancer: a prospective, longitudinal analysis from the St Jude Lifetime Cohort Study.Lancet Oncol. 2024 Jun;25(6):811-822. doi: 10.1016/S1470-2045(24)00157-8. Lancet Oncol. 2024. PMID: 38821086 Free PMC article.
References
-
- Gatta G., Botta L., Rossi S. Childhood cancer survival in Europe 1999-2007: results of EUROCARE-5—a population-based study. Lancet Oncol. 2014;15:35–47. - PubMed
-
- Oeffinger K.C., Mertens A.C., Sklar C.A. Chronic health conditions in adult survivors of childhood cancer. N Engl J Med. 2006;355:1572–1582. - PubMed
-
- van der Pal H.J., van Dalen E.C., van Delden E. High risk of symptomatic cardiac events in childhood cancer survivors. J Clin Oncol. 2012;30:1429–1437. - PubMed
LinkOut - more resources
Full Text Sources
