

Arterial Thromboembolism in Cancer Patients: A Danish Population-Based Cohort Study
- PMID: 34396325
- PMCID: PMC8352038
- DOI: 10.1016/j.jaccao.2021.02.007
Arterial Thromboembolism in Cancer Patients: A Danish Population-Based Cohort Study
Abstract
Background: The relation between cancer and arterial thromboembolism (ATE) remains unclear.
Objectives: The purpose of this study was to evaluate ATE risk in cancer patients.
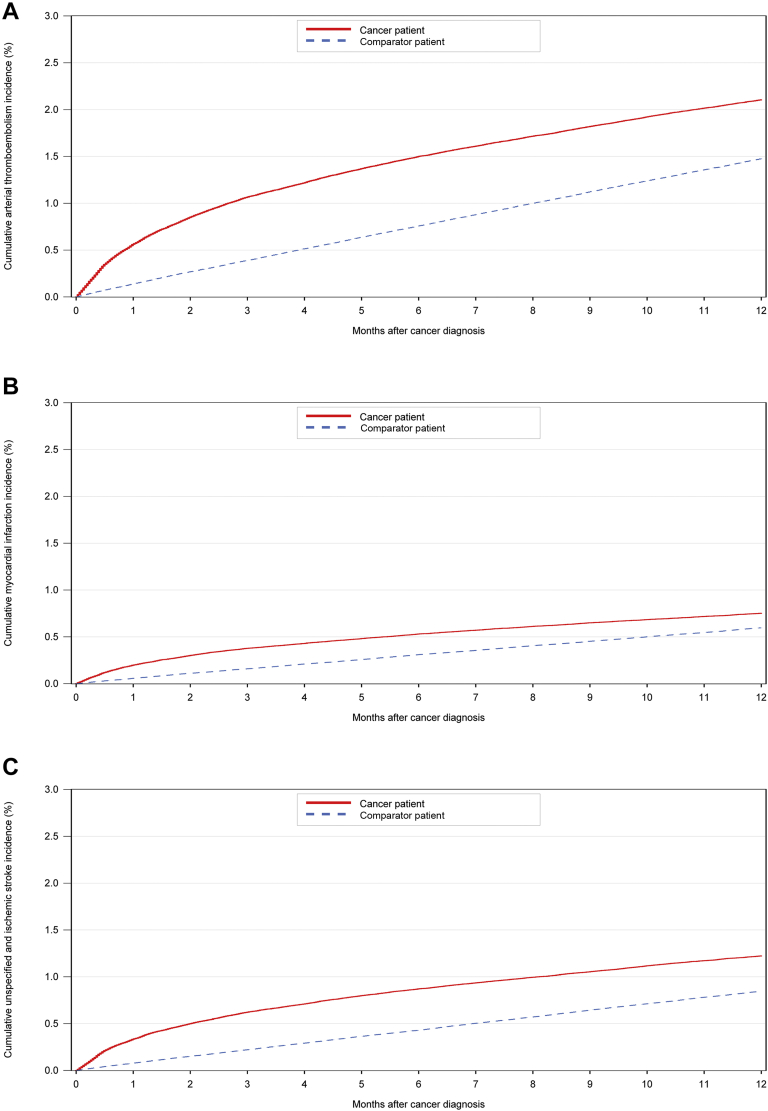
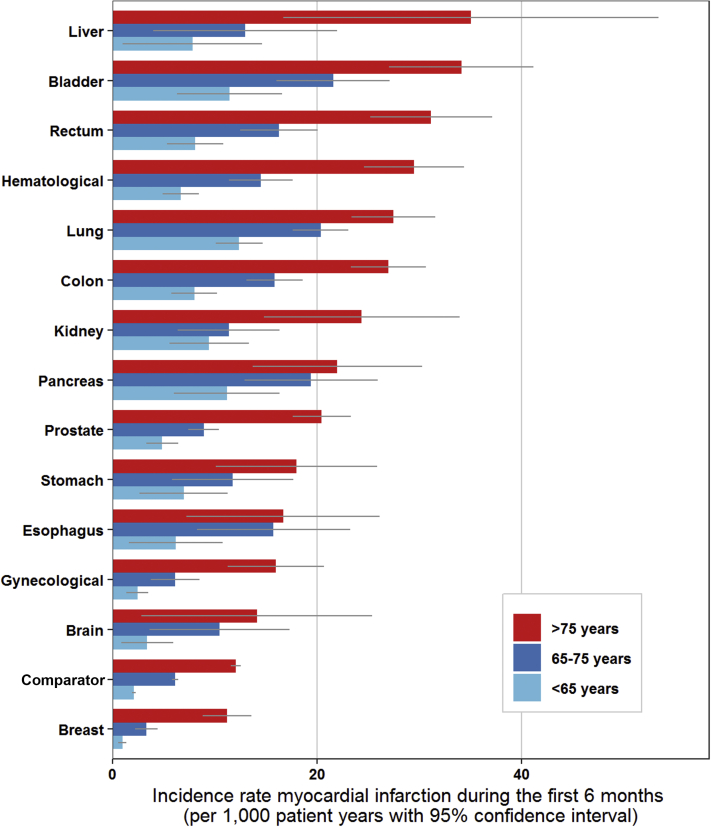
Methods: Danish registries were used to identify all cancer patients between 1997 and 2017, each matched to three cancer-free comparator individuals. ATE was defined as the composite of myocardial infarction, ischemic/unspecified stroke, and peripheral arterial occlusion. A competing risk approach was used to compute cumulative incidences and subdistribution hazard ratios (SHRs). Cause-specific hazard ratios (HRs) were calculated using Cox regression. Among cancer patients, mortality risk was estimated in Cox regression analysis by treating ATE as a time-varying exposure. Patients were followed for 12 months.
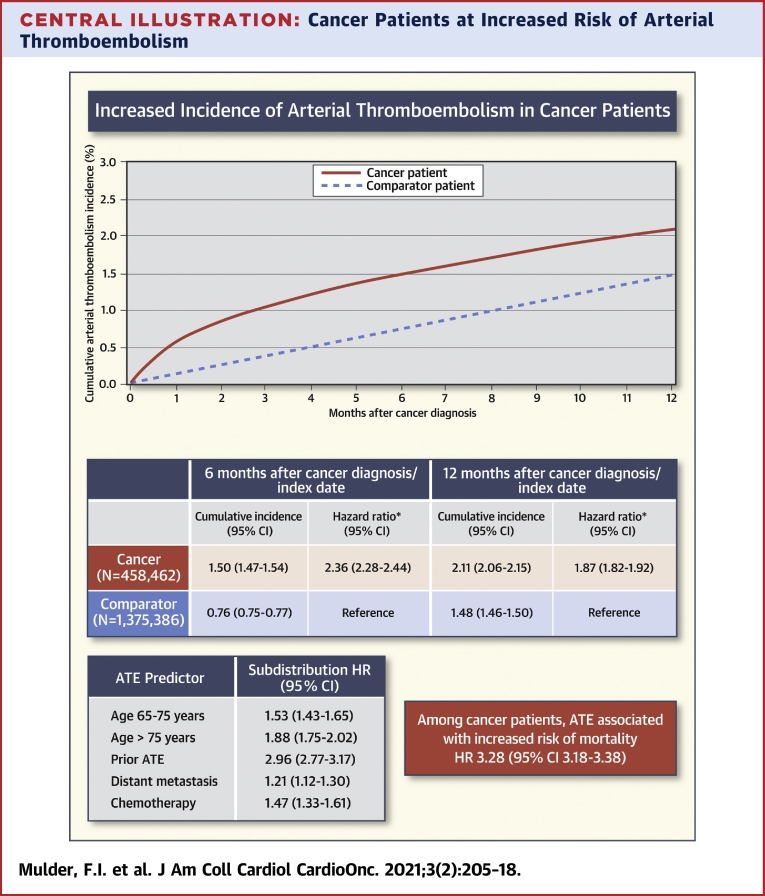
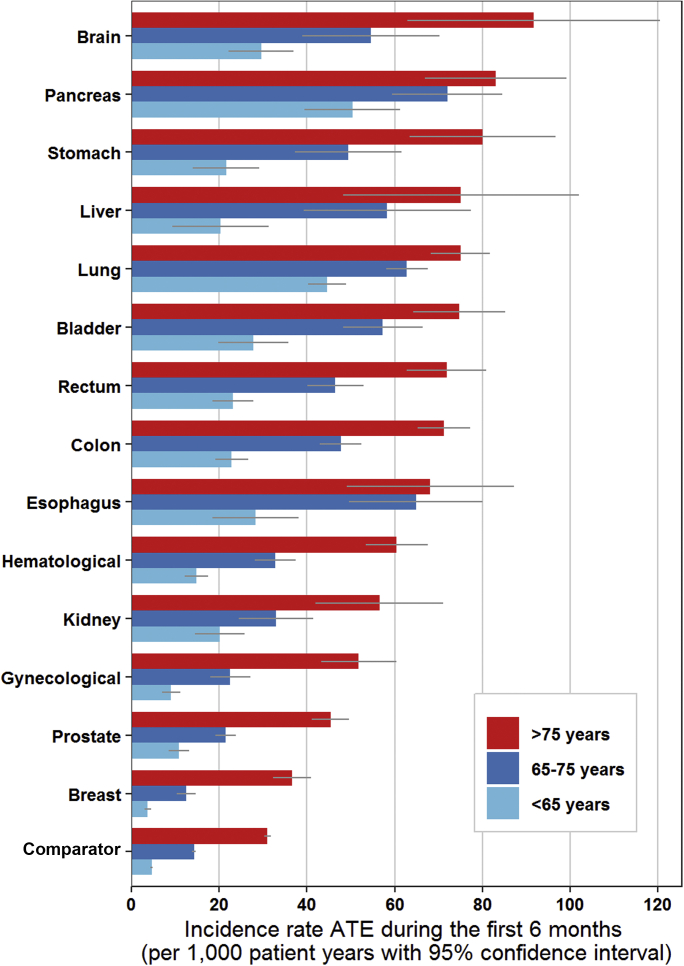
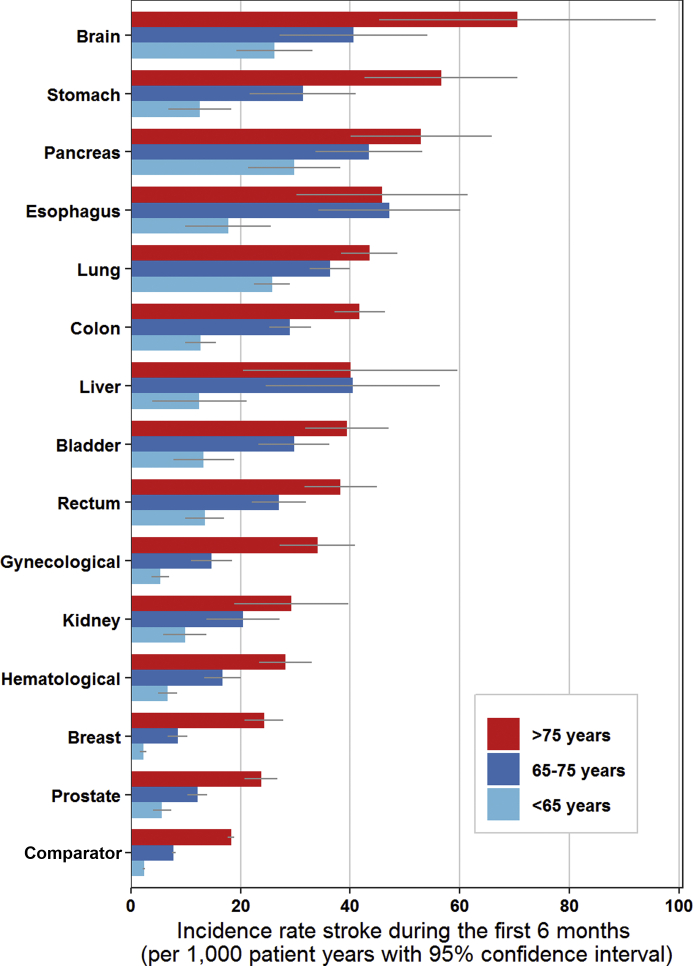
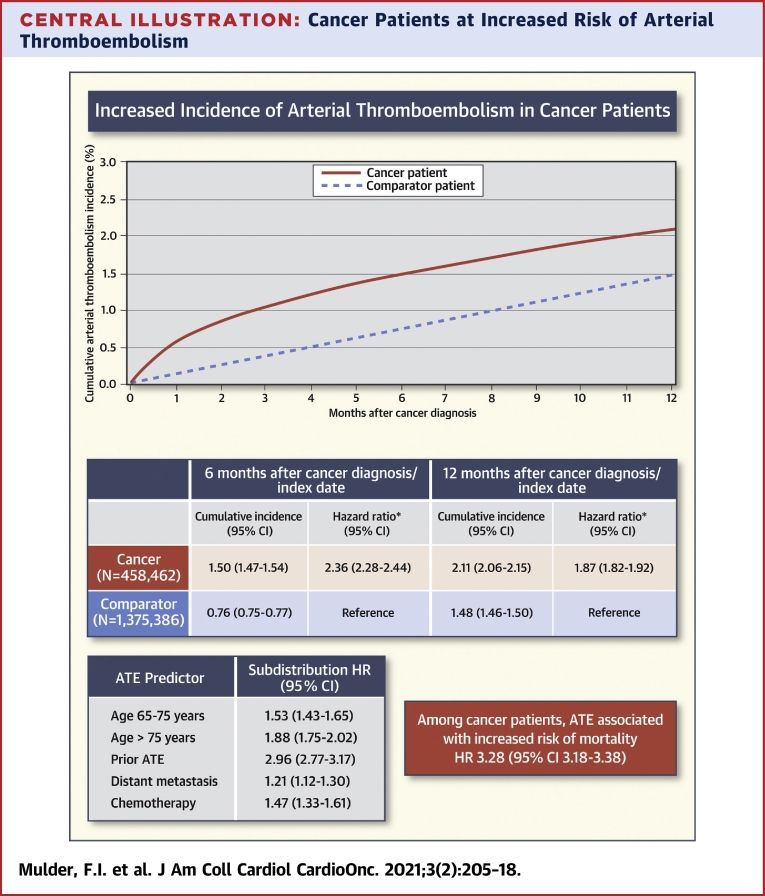
Results: The study included 458,462 cancer patients and 1,375,386 comparator individuals. In the 6-month period following cancer diagnosis/index date, the cumulative incidence for ATE was 1.50% (95% confidence interval [CI]: 1.47% to 1.54%) in cancer patients and 0.76% (95% CI: 0.75% to 0.77%) in comparator individuals (HR: 2.36; 95% CI: 2.28 to 2.44). Among cancer patients age <65 years, 65 to 75 years, and >75 years, this was 0.79% (95% CI: 0.74% to 0.83%), 1.61% (95% CI: 1.55% to 1.67%), and 2.30% (95% CI: 2.22% to 2.38%), respectively. Other predictors for ATE among cancer patients were prior ATE (SHR: 2.96; 95% CI: 2.77 to 3.17), distant metastasis (adjusted SHR: 1.21; 95% CI: 1.12 to 1.30), and chemotherapy (SHR: 1.47; 95% CI: 1.33 to 1.61). Among cancer patients, ATE was associated with an increased risk of mortality (HR: 3.28; 95% CI: 3.18 to 3.38).
Conclusions: Cancer patients are at increased risk of ATE. Clinicians should be aware of this risk, which is associated with mortality.
Keywords: CI, confidence interval; HR, hazard ratio; SHR, subdistribution hazard ratio; arterial occlusion; arterial thromboembolism; cancer; cohort study; ischemic stroke; myocardial infarction; neoplasm.
© 2021 The Authors.
Conflict of interest statement
The Department of Clinical Epidemiology at Aarhus University receives funding for other studies from companies in the form of research grants to (and administered by) Aarhus University. None of these studies has any relation to the present study. This study was supported by a research grant of the Karen Elise Jensen’s Foundation. Dr. van Es is supported by an Amsterdam Cardiovascular Sciences MD/Postdoc grant. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Trousseau A. New Sydenham Society; Paris. London, England: 1865. Plegmasia alba dolens. Lectures on clinical medicine, delivered at the Hotel-Dieu; pp. 281–332.
-
- Graus F., Rogers L.R., Posner J.B. Cerebrovascular complications in patients with cancer. Medicine (Baltimore) 1985;64:16–35. - PubMed
-
- Aleman B.M.P., Van Den Belt-Dusebout A.W., De Bruin M.L. Late cardiotoxicity after treatment for Hodgkin lymphoma. Blood. 2007;109:1878–1886. - PubMed
-
- De Bruin M.L., Dorresteijn L.D.A., Van’t Veer M.B. Increased risk of stroke and transient ischemic attack in 5-year survivors of Hodgkin lymphoma. J Natl Cancer Inst. 2009;101:928–937. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
