

Risk of Atrial Fibrillation According to Cancer Type: A Nationwide Population-Based Study
- PMID: 34396327
- PMCID: PMC8352078
- DOI: 10.1016/j.jaccao.2021.03.006
Risk of Atrial Fibrillation According to Cancer Type: A Nationwide Population-Based Study
Abstract
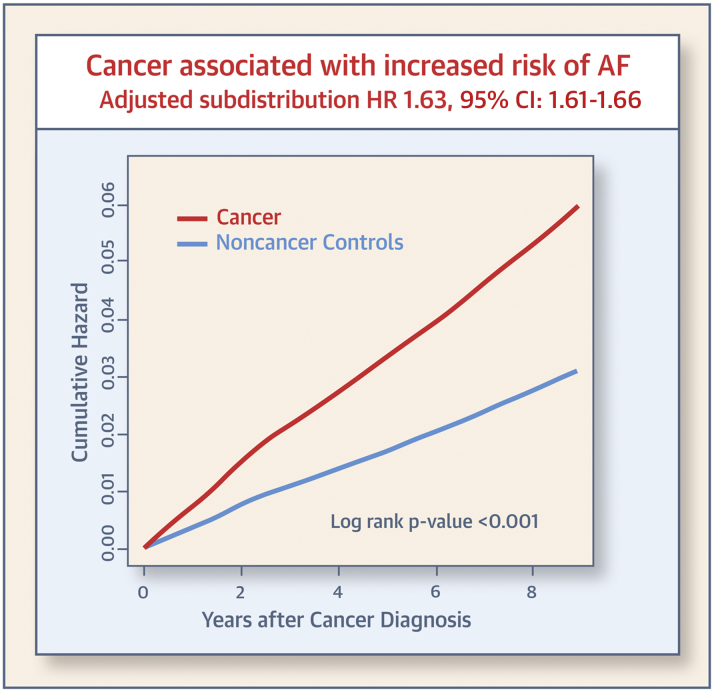
Background: Patients with cancer have an increased risk of atrial fibrillation (AF). However, there is a paucity of information regarding the association between cancer type and risk of AF.
Objectives: This study sought to evaluate the risk of AF according to the type of cancer.
Methods: We enrolled 816,811 patients who were diagnosed with cancer from the Korean National Health Insurance Service database between 2009 and 2016. Age- and sex-matched noncancer control subjects (1:2; n = 1,633,663) were also selected. Newly diagnosed AF was identified based on the type of cancer.
Results: During a median follow-up of 4.5 years, AF was newly diagnosed in 25,356 patients with cancer (6.6 per 1,000 person-years). In multivariable Fine and Gray's regression analysis, cancer was an independent risk factor for incident AF (adjusted subdistribution hazard ratio [aHR]: 1.63; 95% confidence interval [CI]: 1.61 to 1.66). Multiple myeloma showed a higher association with incident AF (aHR: 3.34; 95% CI: 2.98 to 3.75). Esophageal cancer showed the highest risk among solid cancers (aHR: 2.69; 95% CI: 2.45 to 2.95), and stomach cancer showed the lowest association with AF risk (aHR: 1.27; 95% CI 1.23 to 1.32).
Conclusions: Although patients with cancer were found to have a higher risk of AF, the impact on AF development varied by cancer type.
Keywords: AF, atrial fibrillation; CI, confidence interval; CKD, chronic kidney disease; CNS, central nervous system; CVD, cardiovascular disease; DM, diabetes mellitus; HR, hazard ratio; ICD-10, International Classification of Diseases–10th Revision; IQR, interquartile range; NHIS, National Health Insurance Service; atrial fibrillation; cancer; epidemiology; type of cancer.
© 2021 The Authors.
Conflict of interest statement
This work was supported by the Korea Medical Device Development Fund grant funded by the Korean government (the Ministry of Science and ICT; the Ministry of Trade, Industry and Energy; the Ministry of Health and Welfare; the Ministry of Food and Drug Safety) (Project Number: 202013B14) and by the Korea National Research Foundation funded by the Ministry of Education, Science and Technology (grant 2020R1F1A106740). The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures





References
LinkOut - more resources
Full Text Sources
