

Genotype-Phenotype Relations for the Atypical Parkinsonism Genes: MDSGene Systematic Review
- PMID: 34396589
- PMCID: PMC9070562
- DOI: 10.1002/mds.28517
Genotype-Phenotype Relations for the Atypical Parkinsonism Genes: MDSGene Systematic Review
Abstract
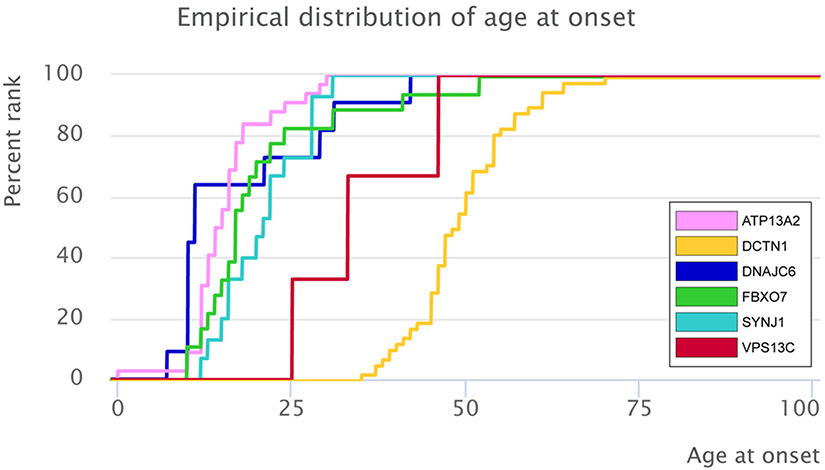
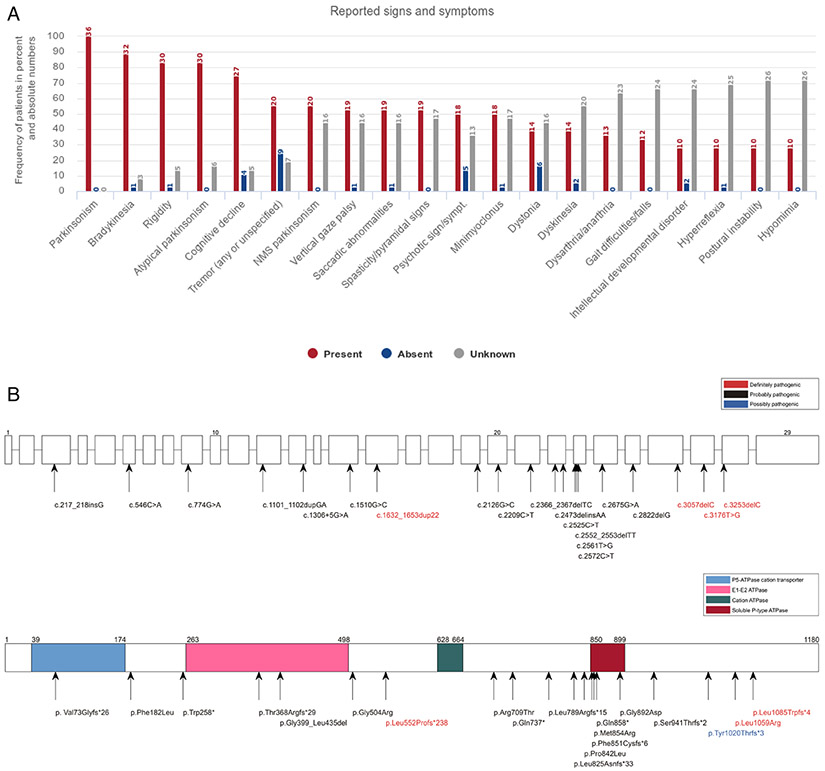
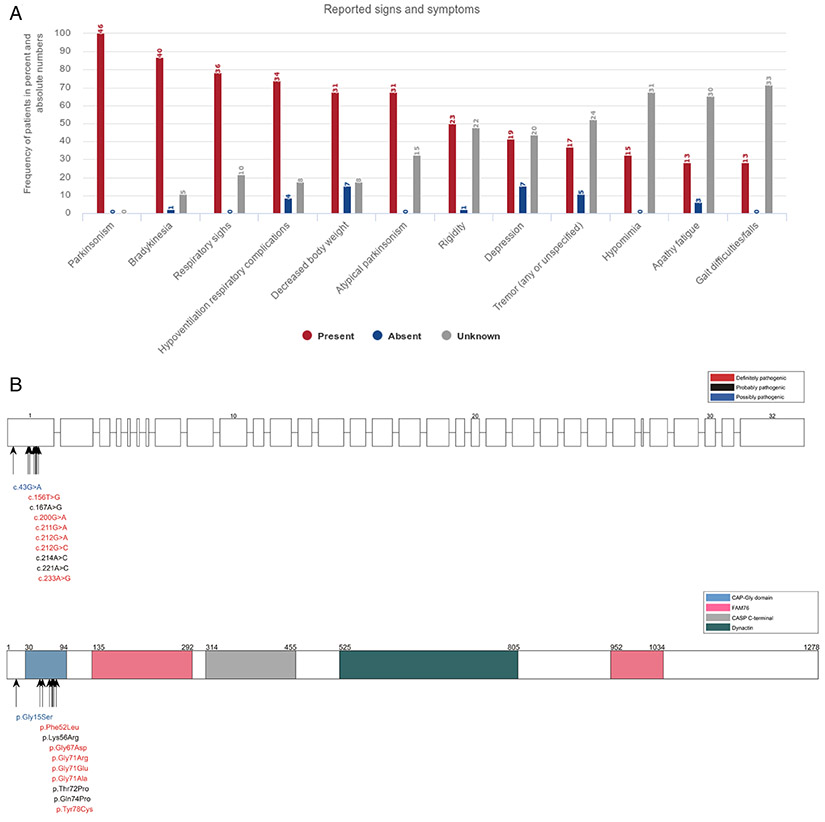
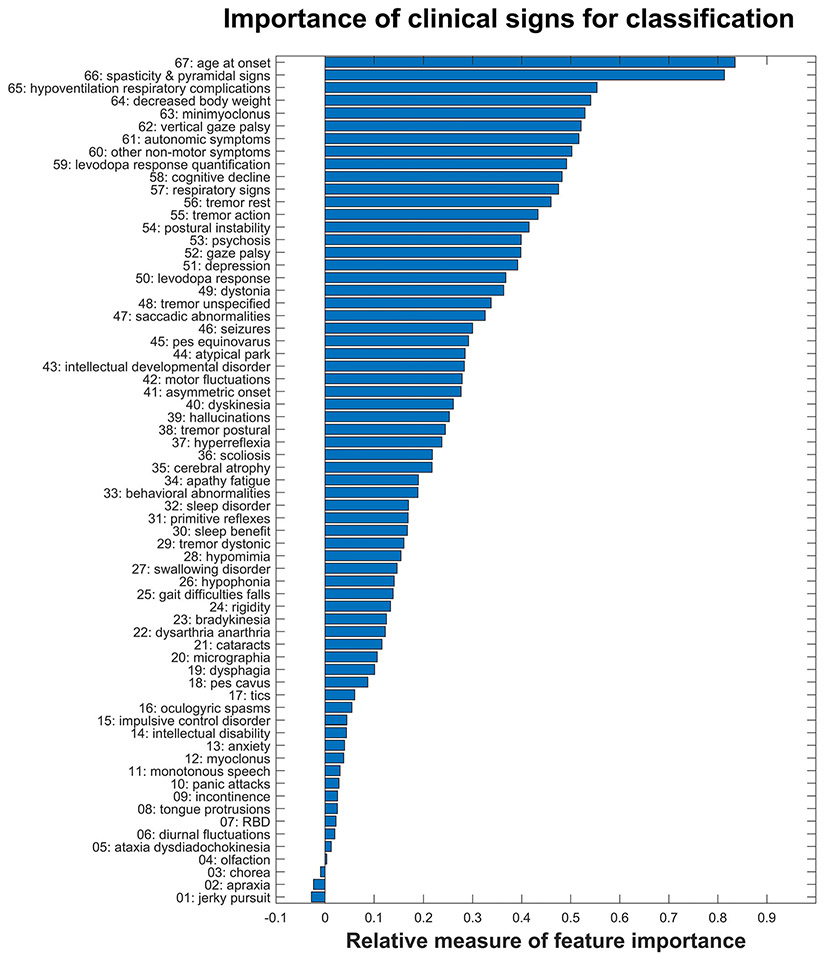
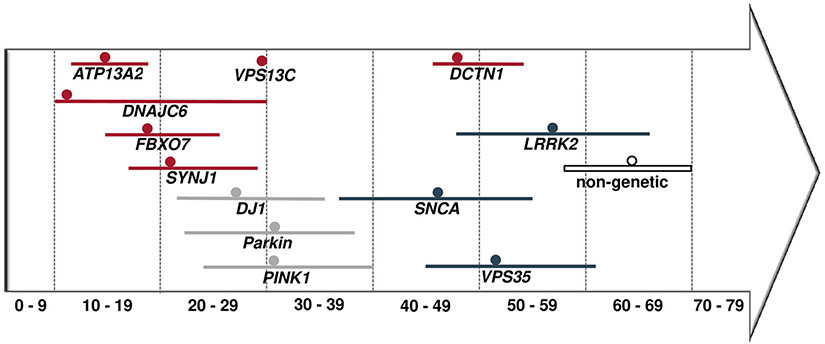
This Movement Disorder Society Genetic mutation database Systematic Review focuses on monogenic atypical parkinsonism with mutations in the ATP13A2, DCTN1, DNAJC6, FBXO7, SYNJ1, and VPS13C genes. We screened 673 citations and extracted genotypic and phenotypic data for 140 patients (73 families) from 77 publications. In an exploratory fashion, we applied an automated classification procedure via an ensemble of bootstrap-aggregated ("bagged") decision trees to distinguish these 6 forms of monogenic atypical parkinsonism and found a high accuracy of 86.5% (95%CI, 86.3%-86.7%) based on the following 10 clinical variables: age at onset, spasticity and pyramidal signs, hypoventilation, decreased body weight, minimyoclonus, vertical gaze palsy, autonomic symptoms, other nonmotor symptoms, levodopa response quantification, and cognitive decline. Comparing monogenic atypical with monogenic typical parkinsonism using 2063 data sets from Movement Disorder Society Genetic mutation database on patients with SNCA, LRRK2, VPS35, Parkin, PINK1, and DJ-1 mutations, the age at onset was earlier in monogenic atypical parkinsonism (24 vs 40 years; P = 1.2647 × 10-12) and levodopa response less favorable than in patients with monogenic typical presentations (49% vs 93%). In addition, we compared monogenic to nonmonogenic atypical parkinsonism using data from 362 patients with progressive supranuclear gaze palsy, corticobasal degeneration, multiple system atrophy, or frontotemporal lobar degeneration. Although these conditions share many clinical features with the monogenic atypical forms, they can typically be distinguished based on their later median age at onset (64 years; IQR, 57-70 years). In conclusion, age at onset, presence of specific signs, and degree of levodopa response inform differential diagnostic considerations and genetic testing indications in atypical forms of parkinsonism. © 2021 International Parkinson and Movement Disorder Society.
Keywords: MDSGene; Parkinson's disease; atypical parkinsonism; genetics; red flags; systematic review.
© 2021 International Parkinson and Movement Disorder Society.
Conflict of interest statement
Figures
References
-
- Trinh J, Zeldenrust FMJ, Huang J, et al. Genotype-phenotype relations for the Parkinson’s disease genes SNCA, LRRK2, VPS35: MDSGene systematic review. Mov Disord 2018;33(12):1857–1870. - PubMed
-
- Kasten M, Hartmann C, Hampf J, et al. Genotype-phenotype relations for the Parkinson’s disease genes Parkin, PINK1, DJ1: MDSGene systematic review. Mov Disord 2018;33(5):730–741. - PubMed
-
- Lill CM, Mashychev A, Hartmann C, et al. Launching the movement disorders society genetic mutation database (MDSGene). Mov Disord 2016;31(5):607–609. - PubMed
-
- Weissbach A, Wittke C, Kasten M, Klein C. Atypical’ Parkinson’s disease - genetic. Int Rev Neurobiol 2019;149:207–235. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
