

Survival of COVID-19 Patients With Respiratory Failure is Related to Temporal Changes in Gas Exchange and Mechanical Ventilation
- PMID: 34397301
- PMCID: PMC8442134
- DOI: 10.1177/08850666211033836
Survival of COVID-19 Patients With Respiratory Failure is Related to Temporal Changes in Gas Exchange and Mechanical Ventilation
Abstract
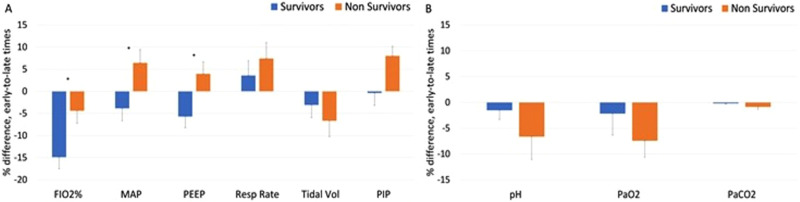
Background: Respiratory failure due to coronavirus disease of 2019 (COVID-19) often presents with worsening gas exchange over a period of days. Once patients require mechanical ventilation (MV), the temporal change in gas exchange and its relation to clinical outcome is poorly described. We investigated whether gas exchange over the first 5 days of MV is associated with mortality and ventilator-free days at 28 days in COVID-19. Methods: In a cohort of 294 COVID-19 patients, we used data during the first 5 days of MV to calculate 4 daily respiratory scores: PaO2/FiO2 (P/F), oxygenation index (OI), ventilatory ratio (VR), and Murray lung injury score. The association between these scores at early (days 1-3) and late (days 4-5) time points with mortality was evaluated using logistic regression, adjusted for demographics. Correlation with ventilator-free days was assessed (Spearman rank-order coefficients). Results: Overall mortality was 47.6%. Nonsurvivors were older (P < .0001), more male (P = .029), with more preexisting cardiopulmonary disease compared to survivors. Mean PaO2 and PaCO2 were similar during this timeframe. However, by days 4 to 5 values for all airway pressures and FiO2 had diverged, trending lower in survivors and higher in nonsurvivors. The most substantial between-group difference was the temporal change in OI, improving 15% in survivors and worsening 11% in nonsurvivors (P < .05). The adjusted mortality OR was significant for age (1.819, P = .001), OI at days 4 to 5 (2.26, P = .002), and OI percent change (1.90, P = .02). The number of ventilator-free days correlated significantly with late VR (-0.166, P < .05), early and late OI (-0.216, P < .01; -0.278, P < .01, respectively) and early and late P/F (0.158, P < .05; 0.283, P < .01, respectively). Conclusion: Nonsurvivors of COVID-19 needed increasing intensity of MV to sustain gas exchange over the first 5 days, unlike survivors. Temporal change OI, reflecting both PaO2 and the intensity of MV, is a potential marker of outcome in respiratory failure due to COVID-19.
Keywords: COVID-19; ICU outcomes; Murray lung injury score; mechanical ventilation; oxygenation index; ventilatory ratio.
Conflict of interest statement
Figures



References
-
- https://www.who.int/publications/m/item/weekly-epidemiological-update---.... Accessed January 8, 2020.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
