

Comparison of a Single-Session Pain Management Skills Intervention With a Single-Session Health Education Intervention and 8 Sessions of Cognitive Behavioral Therapy in Adults With Chronic Low Back Pain: A Randomized Clinical Trial
- PMID: 34398206
- PMCID: PMC8369357
- DOI: 10.1001/jamanetworkopen.2021.13401
Comparison of a Single-Session Pain Management Skills Intervention With a Single-Session Health Education Intervention and 8 Sessions of Cognitive Behavioral Therapy in Adults With Chronic Low Back Pain: A Randomized Clinical Trial
Erratum in
-
Clarification of Conflict of Interest Disclosure.JAMA Netw Open. 2022 Apr 1;5(4):e229739. doi: 10.1001/jamanetworkopen.2022.9739. JAMA Netw Open. 2022. PMID: 35385097 Free PMC article. No abstract available.
Abstract
Importance: Chronic low back pain (CLBP), the most prevalent chronic pain condition, imparts substantial disability and discomfort. Cognitive behavioral therapy (CBT) reduces the effect of CLBP, but access is limited.
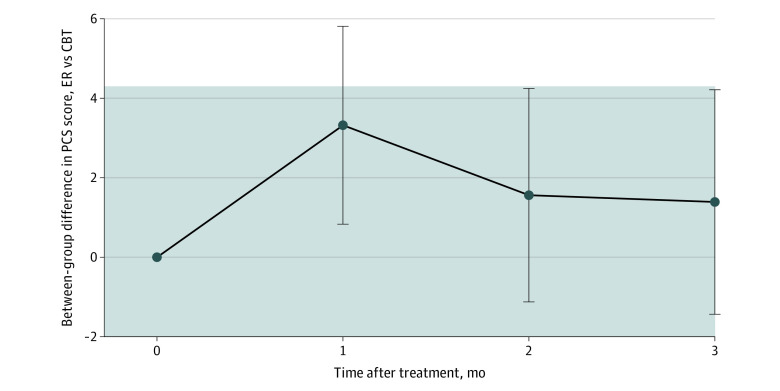
Objective: To determine whether a single class in evidence-based pain management skills (empowered relief) is noninferior to 8-session CBT and superior to health education at 3 months after treatment for improving pain catastrophizing, pain intensity, pain interference, and other secondary outcomes.
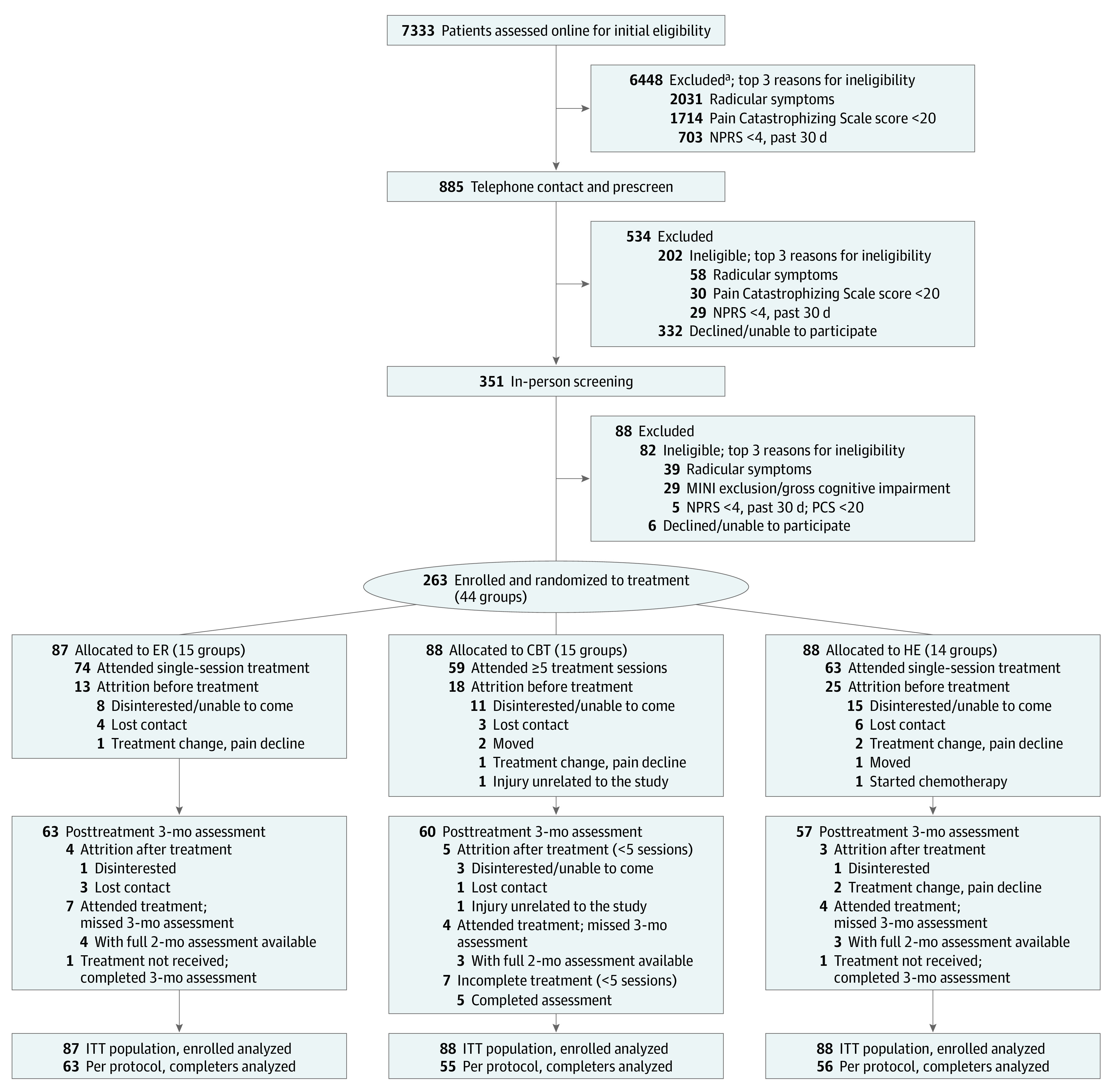
Design, setting, and participants: This 3-arm randomized clinical trial collected data from May 24, 2017, to March 3, 2020. Participants included individuals in the community with self-reported CLBP for 6 months or more and an average pain intensity of at least 4 (range, 0-10, with 10 indicating worst pain imaginable). Data were analyzed using intention-to-treat and per-protocol approaches.
Interventions: Participants were randomized to (1) empowered relief, (2) health education (matched to empowered relief for duration and format), or (3) 8-session CBT. Self-reported data were collected at baseline, before treatment, and at posttreatment months 1, 2, and 3.
Main outcomes and measures: Group differences in Pain Catastrophizing Scale scores and secondary outcomes at month 3 after treatment. Pain intensity and pain interference were priority secondary outcomes.
Results: A total of 263 participants were included in the analysis (131 women [49.8%], 130 men [49.4%], and 2 other [0.8%]; mean [SD] age, 47.9 [13.8] years) and were randomized into 3 groups: empowered relief (n = 87), CBT (n = 88), and health education (n = 88). Empowered relief was noninferior to CBT for pain catastrophizing scores at 3 months (difference from CBT, 1.39 [97.5% CI, -∞ to 4.24]). Empowered relief and CBT were superior to health education for pain catastrophizing scores (empowered relief difference from health education, -5.90 [95% CI, -8.78 to -3.01; P < .001]; CBT difference from health education, -7.29 [95% CI, -10.20 to -4.38; P < .001]). Pain catastrophizing score reductions for empowered relief and CBT at 3 months after treatment were clinically meaningful (empowered relief, -9.12 [95% CI, -11.6 to -6.67; P < .001]; CBT, -10.94 [95% CI, -13.6 to -8.32; P < .001]; health education, -4.60 [95% CI, -7.18 to -2.01; P = .001]). Between-group comparisons for pain catastrophizing at months 1 to 3 were adjusted for baseline pain catastrophizing scores and used intention-to-treat analysis. Empowered relief was noninferior to CBT for pain intensity and pain interference (priority secondary outcomes), sleep disturbance, pain bothersomeness, pain behavior, depression, and anxiety. Empowered relief was inferior to CBT for physical function.
Conclusions and relevance: Among adults with CLBP, a single-session pain management class resulted in clinically significant improvements in pain catastrophizing, pain intensity, pain interference, and other secondary outcomes that were noninferior to 8-session CBT at 3 months.
Trial registration: ClinicalTrials.gov Identifier: NCT03167086.
Conflict of interest statement
Figures
References
-
- Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. National Academies Press; 2011. - PubMed
-
- Turner JA, Anderson ML, Balderson BH, Cook AJ, Sherman KJ, Cherkin DC. Mindfulness-based stress reduction and cognitive behavioral therapy for chronic low back pain: similar effects on mindfulness, catastrophizing, self-efficacy, and acceptance in a randomized controlled trial. Pain. 2016;157(11):2434-2444. doi:10.1097/j.pain.0000000000000635 - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
