

The Chagas disease study landscape: A systematic review of clinical and observational antiparasitic treatment studies to assess the potential for establishing an individual participant-level data platform
- PMID: 34398888
- PMCID: PMC8428795
- DOI: 10.1371/journal.pntd.0009697
The Chagas disease study landscape: A systematic review of clinical and observational antiparasitic treatment studies to assess the potential for establishing an individual participant-level data platform
Abstract
Background: Chagas disease (CD), caused by the parasite Trypanosoma cruzi, affects ~6-7 million people worldwide. Significant limitations still exist in our understanding of CD. Harnessing individual participant data (IPD) from studies could support more in-depth analyses to address the many outstanding research questions. This systematic review aims to describe the characteristics and treatment practices of clinical studies in CD and assess the breadth and availability of research data for the potential establishment of a data-sharing platform.
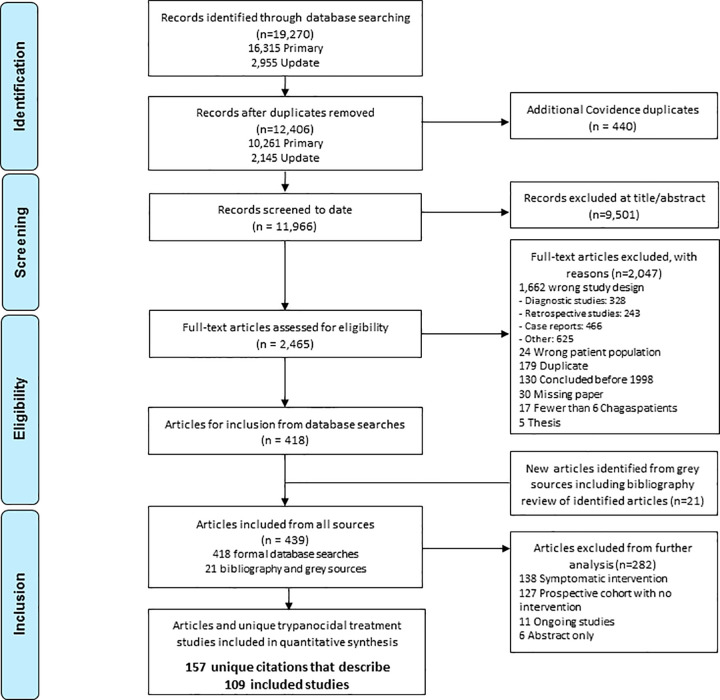
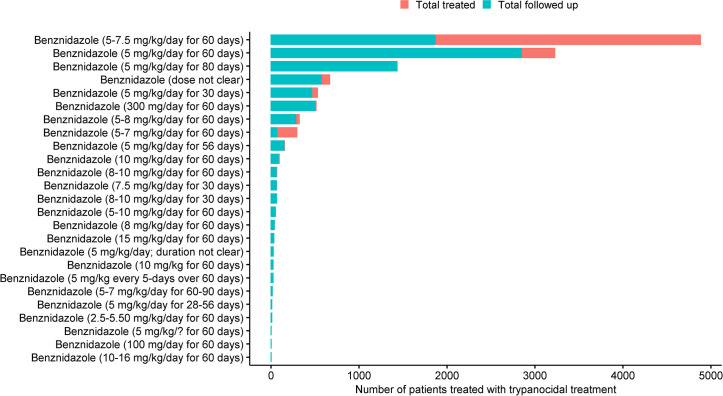
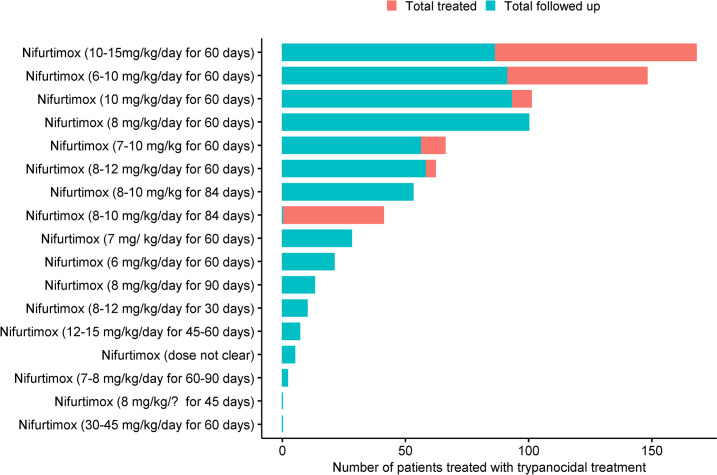
Methodology/principal findings: This review includes prospective CD clinical studies published after 1997 with patients receiving a trypanocidal treatment. The following electronic databases and clinical trial registry platforms were searched: Cochrane Library, PubMed, Embase, LILACS, Scielo, Clintrials.gov, and WHO ICTRP. Of the 11,966 unique citations screened, 109 (0.9%) studies (31 observational and 78 interventional) representing 23,116 patients were included. Diagnosis for patient enrolment required 1 positive test result in 5 (4.6%) studies (2 used molecular method, 1 used molecular and serology, 2 used serology and parasitological methods), 2 in 60 (55.0%), 3 in 14 (12.8%) and 4 or more in 4 (3.7%) studies. A description of treatment regimen was available for 19,199 (83.1%) patients, of whom 14,605 (76.1%) received an active treatment and 4,594 (23.9%) were assigned to a placebo/no-treatment. Of the 14,605 patients who received an active treatment, benznidazole was administered in 12,467 (85.4%), nifurtimox in 825 (5.6%), itraconazole in 284 (1.9%), allopurinol in 251 (1.7%) and other drugs in 286 (1.9%). Assessment of efficacy varied largely and was based primarily on biological outcome; parasitological efficacy relied on serology in 67/85 (78.8%) studies, molecular methods in 52/85 (61.2%), parasitological in 34/85 (40.0%), microscopy in 3/85 (3.5%) and immunohistochemistry in 1/85 (1.2%). The median time at which parasitological assessment was carried out was 79 days [interquartile range (IQR): 30-180] for the first assessment, 180 days [IQR: 60-500] for second, and 270 days [IQR: 18-545] for the third assessment.
Conclusions/significance: This review demonstrates the heterogeneity of clinical practice in CD treatment and in the conduct of clinical studies. The sheer volume of potential IPD identified demonstrates the potential for development of an IPD platform for CD and that such efforts would enable in-depth analyses to optimise the limited pharmacopoeia of CD and inform prospective data collection.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- World Health Organization. WHO fact sheet no. 340. 2016. [cited 1 Sep 2016]. Available: http://www.who.int/mediacentre/factsheets/fs340/en/.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
