

Spotlight on laparoscopy in the surgical resection of locally advanced rectal cancer: multicenter propensity score match study
- PMID: 34399445
- PMCID: PMC9441543
- DOI: 10.3393/ac.2020.01060.0151
Spotlight on laparoscopy in the surgical resection of locally advanced rectal cancer: multicenter propensity score match study
Abstract
Purpose: This study was aimed to assess the feasibility of laparoscopic rectal surgery, comparing quality of surgical specimen, morbidity, and mortality.
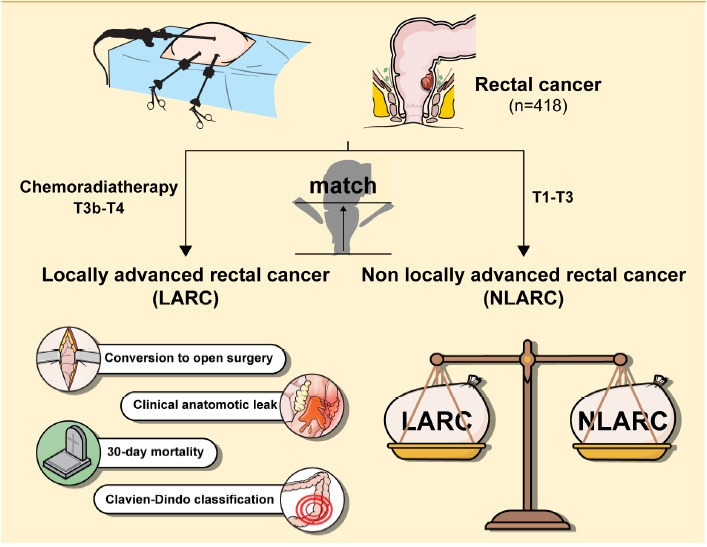
Methods: Prospectively acquired data from consecutive patients undergoing laparoscopic surgery for rectal cancer, at 2 minimally invasive colorectal units, operated by the same team was included. Locally advanced rectal tumors were identified as T3B or T4 with preoperative magnetic resonance imaging scans. All the patients were operated on by the same team. The 1:1 propensity score matching was performed to create a perfect match in terms of tumor height.
Results: Total of 418 laparoscopic resections were performed, out of which 109 patients had locally advanced rectal cancer (LARC) and were propensity score matched with non-LARC (NLARC) patients. Median operation time was higher for the LARC group (270 minutes vs. 250 minutes, P=0.011). However, conversion to open surgery was done in 5 vs. 2 patients (P=0.445), reoperation in 8 vs. 7 (P=0.789), clinical anastomotic leak was found in 3 vs. 2 (P=0.670), and 30-day mortality rates was 2 vs. 1 (P>0.999) between LARC and NLARC, respectively. Readmission rate was higher in the NLARC group (33 patients vs. 19 patients, P=0.026), due to stoma-related issues. There was no statistically significant difference in the R0 resection between the 2 groups (99 patients in LARC vs. 104 patients in NLARC, P=0.284).
Conclusion: This study demonstrates that standardized approach to laparoscopy is safe and feasible in LARC. Comparable postoperative short-term clinical and pathological outcomes were seen between LARC and NLARC groups.
Keywords: Laparoscopic colorectal surgery; Minimally invasive surgical procedures; Rectal neoplasms.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Comment in
-
Advances in surgery for locally advanced rectal cancer.Ann Coloproctol. 2022 Aug;38(4):279-280. doi: 10.3393/ac.2022.00493.0070. Epub 2022 Aug 29. Ann Coloproctol. 2022. PMID: 36059073 Free PMC article. No abstract available.
References
-
- Heald RJ, Husband EM, Ryall RD. The mesorectum in rectal cancer surgery—the clue to pelvic recurrence? Br J Surg. 1982;69:613–6. - PubMed
-
- Kennedy ED, Simunovic M, Jhaveri K, Kirsch R, Brierley J, Drolet S, et al. Safety and feasibility of using magnetic resonance imaging criteria to identify patients with “good prognosis” rectal cancer eligible for primary surgery: the phase 2 nonrandomized QuickSilver clinical trial. JAMA Oncol. 2019;5:961–6. - PMC - PubMed
LinkOut - more resources
Full Text Sources
