

Multi-centre randomised controlled trial comparing arthroscopic hip surgery to physiotherapist-led care for femoroacetabular impingement (FAI) syndrome on hip cartilage metabolism: the Australian FASHIoN trial
- PMID: 34399702
- PMCID: PMC8369620
- DOI: 10.1186/s12891-021-04576-z
Multi-centre randomised controlled trial comparing arthroscopic hip surgery to physiotherapist-led care for femoroacetabular impingement (FAI) syndrome on hip cartilage metabolism: the Australian FASHIoN trial
Abstract
Background: Arthroscopic surgery for femoroacetabular impingement syndrome (FAI) is known to lead to self-reported symptom improvement. In the context of surgical interventions with known contextual effects and no true sham comparator trials, it is important to ascertain outcomes that are less susceptible to placebo effects. The primary aim of this trial was to determine if study participants with FAI who have hip arthroscopy demonstrate greater improvements in delayed gadolinium-enhanced magnetic resonance imaging (MRI) of cartilage (dGEMRIC) index between baseline and 12 months, compared to participants who undergo physiotherapist-led management.
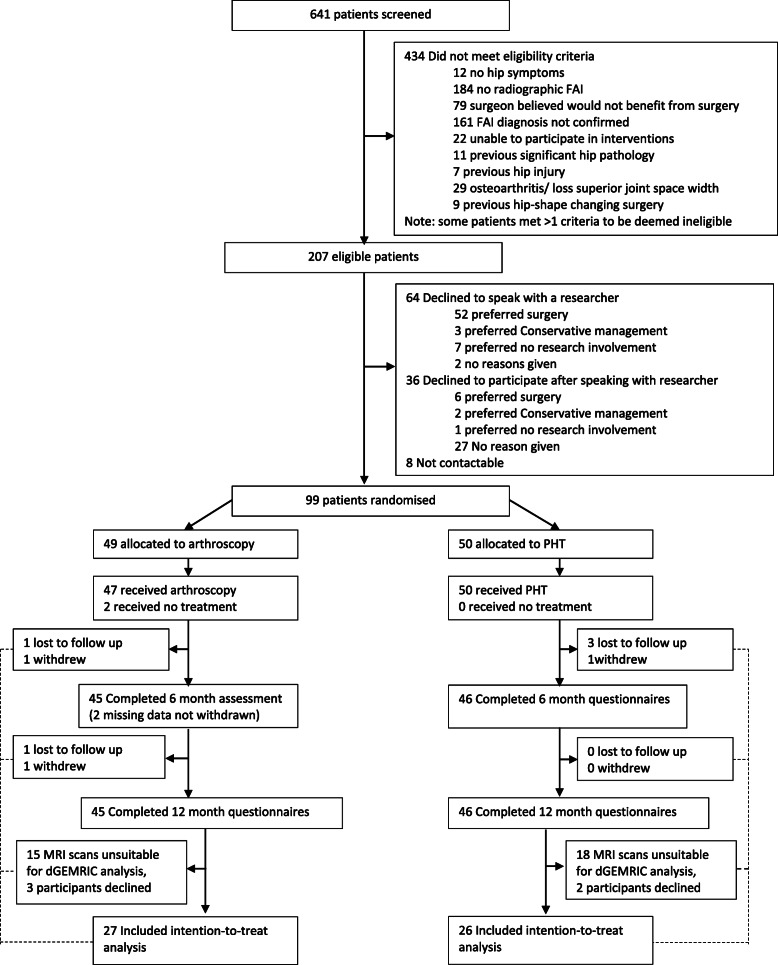
Methods: Multi-centre, pragmatic, two-arm superiority randomised controlled trial comparing physiotherapist-led management to hip arthroscopy for FAI. FAI participants were recruited from participating orthopaedic surgeons clinics, and randomly allocated to receive either physiotherapist-led conservative care or surgery. The surgical intervention was arthroscopic FAI surgery. The physiotherapist-led conservative management was an individualised physiotherapy program, named Personalised Hip Therapy (PHT). The primary outcome measure was change in dGEMRIC score between baseline and 12 months. Secondary outcomes included a range of patient-reported outcomes and structural measures relevant to FAI pathoanatomy and hip osteoarthritis development. Interventions were compared by intention-to-treat analysis.
Results: Ninety-nine participants were recruited, of mean age 33 years and 58% male. Primary outcome data were available for 53 participants (27 in surgical group, 26 in PHT). The adjusted group difference in change at 12 months in dGEMRIC was -59 ms (95%CI - 137.9 to - 19.6) (p = 0.14) favouring PHT. Hip-related quality of life (iHOT-33) showed improvements in both groups with the adjusted between-group difference at 12 months showing a statistically and clinically important improvement in arthroscopy of 14 units (95% CI 5.6 to 23.9) (p = 0.003).
Conclusion: The primary outcome of dGEMRIC showed no statistically significant difference between PHT and arthroscopic hip surgery at 12 months of follow-up. Patients treated with surgery reported greater benefits in symptoms at 12 months compared to PHT, but these benefits are not explained by better hip cartilage metabolism.
Trial registration details: Australia New Zealand Clinical Trials Registry reference: ACTRN12615001177549 . Trial registered 2/11/2015.
Keywords: Arthroscopy; FAI; Femoroacetabular impingement syndrome; Hip; Physiotherapy; Surgery; dGEMRIC.
© 2021. The Author(s).
Conflict of interest statement
DJH is a consultant to Pfizer, Lilly, TLCBio and Merck Serono and is supported by an NHMRC Practitioner Fellowship. KLB was supported by an NHMRC Principal Research Fellowship (APP1058440). SMG acknowledges the support of the Parker-Hughes endowment and the Frecker Family bequest. NEF is an NIHR Senior Investigator in the UK and was supported through an NIHR Research Professorship (NIHR-RP-011-015). MH was supported by a Sir Randal Heymanson Research Fellowship from The University of Melbourne. The rest of the authors do not have any competing interest.
References
-
- Ganz R, Parvizi J, Beck M, Leunig M, Notzli H, Siebenrock KA. Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res. 2003;417:112–120. - PubMed
