

Iliosacral Bone Tumor Resection Using Cannulated Screw-Guided Gigli Saw - A Novel Technique
- PMID: 34399773
- PMCID: PMC8369724
- DOI: 10.1186/s12957-021-02349-5
Iliosacral Bone Tumor Resection Using Cannulated Screw-Guided Gigli Saw - A Novel Technique
Abstract
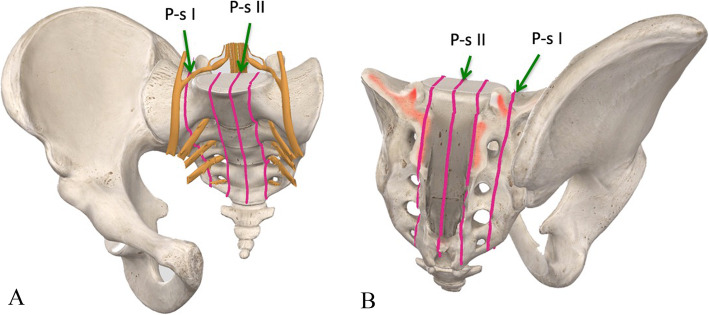
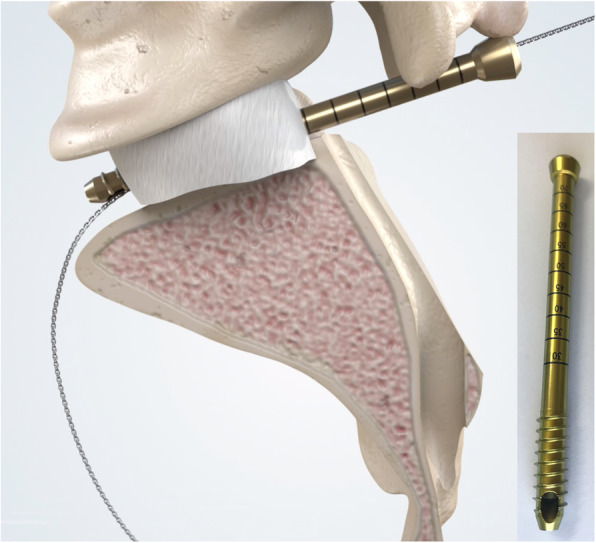
Background: Adequate margins are technically difficult to achieve for malignant tumors involving the sacroiliac joint due to limited accessibility and viewing window. In order to address the technical difficulties faced in iliosacral tumor resection, we proposed a technique for precise osteotomy, which involved the use of canulated screws and Gigli saw (CSGS) that facilitated directional control, anteroposterior linkage of resection points and adequate surgical margins. The purpose of the current study was to evaluate whether CSGS technique facilitated sagittal osteotomy at sacral side, and were adequate surgical margins achieved? Also functional and oncological outcomes was determined along with the noteworthy complications.
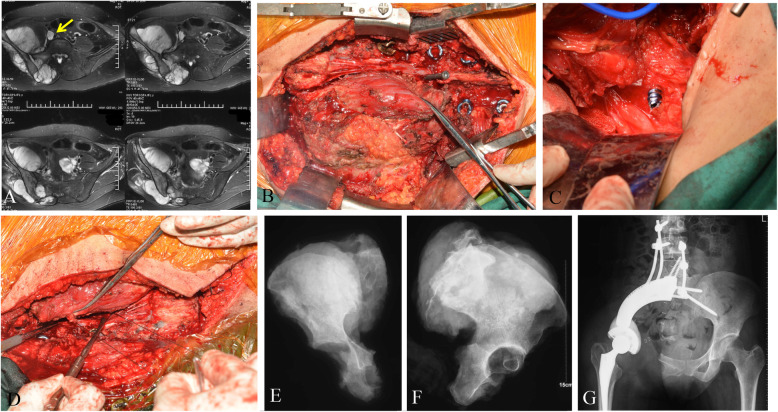
Methods: From April 2018 to November 2019, we retrospectively reviewed 15 patients who underwent resections for primary tumors of pelvis or sacrum necessitating iliosacral joint removal using the proposed CSGS technique. Chondrosarcoma was the most common diagnosis. The osteotomy site within sacrum was at ipsilateral ventral sacral foramina in 8 cases, midline of sacrum in 5 cases, and contralateral ventral sacral foramina and sacral ala with 1 case each. The average intraoperative blood loss was 3640 mL (range, 1200 and 6000 mL) with a mean operation duration of 7.4 hours (range, 5 to 12 hours). The mean follow-up was 23.0 months (range, 18 and 39 months) for alive patients.
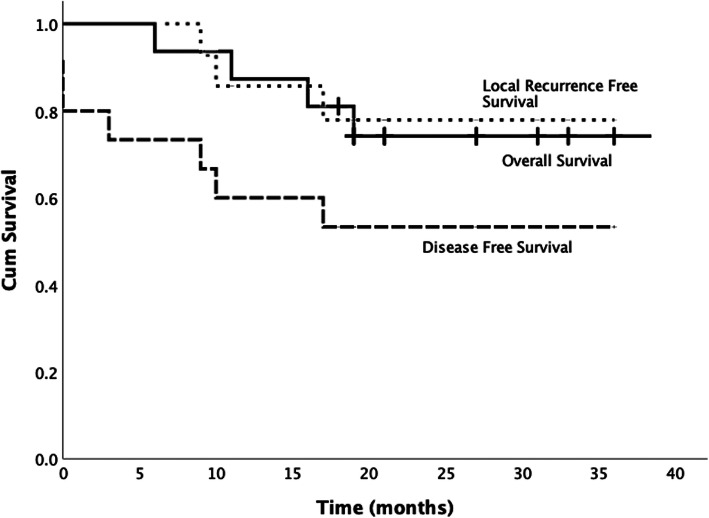
Results: Surgical margins were wide in 12 patients (80%), wide-contaminated in 1 patient (6.7%), and marginal in 2 patients (13.3%). R0 resection was achieved in 12 (80%) patients and R1 resection in 3 patients. There were three local recurrences (20%) occurred at a mean time of 11 months postoperatively. No local recurrence was observed at sacral osteotomy. The overall one-year and three-year survival rate was 86.7% and 72.7% respectively.Complications occurred in three patients.
Conclusions: The current study demonstrated that CSGS technique for tumor resection within the sacrum and pelvis was feasible and can achieve ideal resection accuracies. The use of CSGS was associated with high likelihood of negative margin resections in the current series. Intraoperative use of CSGS appeared to be technically straightforward and allowed achievement of planned surgical margins. It is worthwhile to consider the use of CSGS technique in resection of pelvic tumors with sacral invasion and iliosacral tumors, however further follow-up at mid to long-term is warranted to observe local recurrence rate.
Keywords: iliosacral tumor; limb salvage; osteotomy; surgical margin.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
