

Investigation of the clinical inter-observer bias in prostate fiducial marker image registration between CT and MR images
- PMID: 34399806
- PMCID: PMC8365967
- DOI: 10.1186/s13014-021-01865-8
Investigation of the clinical inter-observer bias in prostate fiducial marker image registration between CT and MR images
Abstract
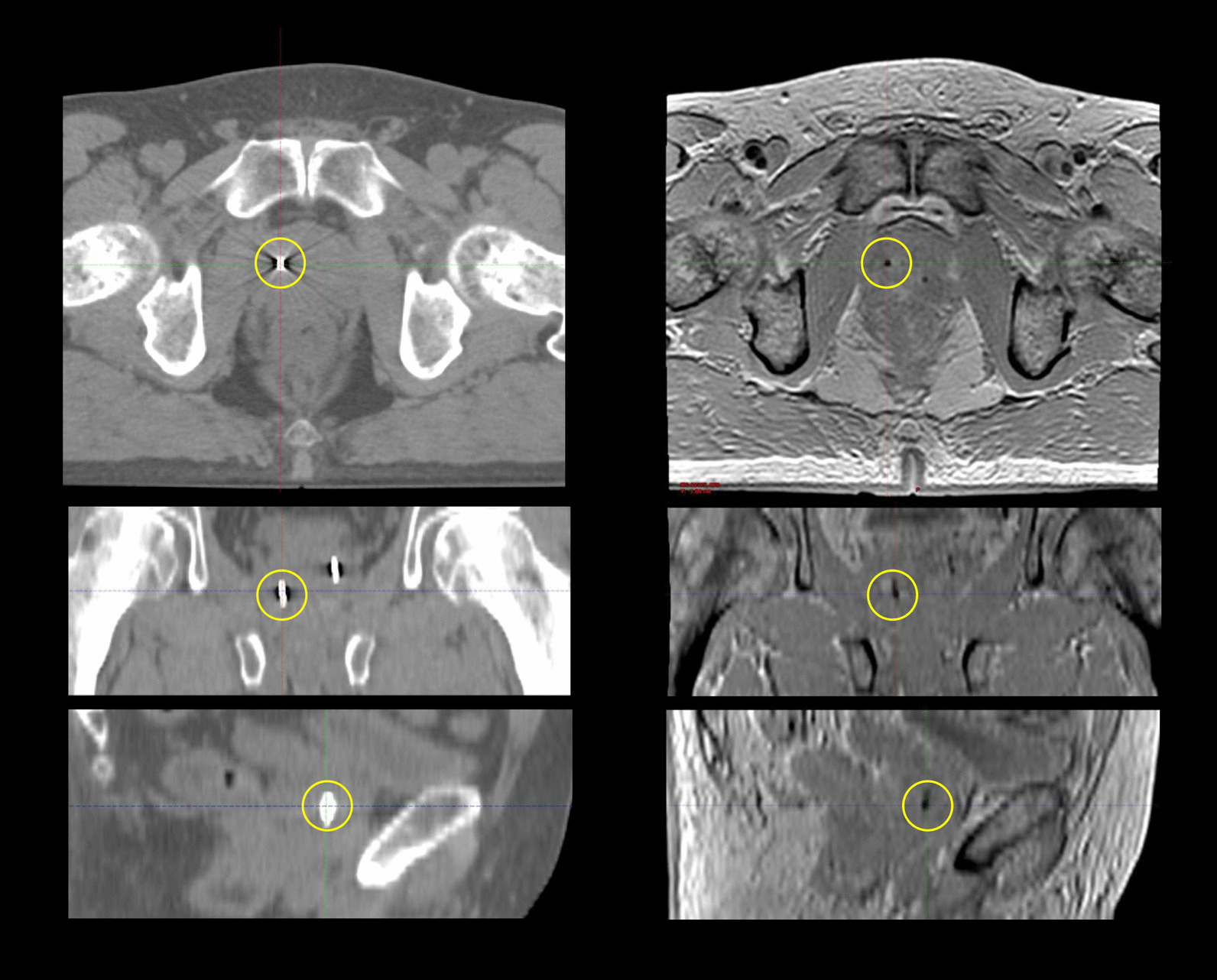
Background and purpose: Inter-modality image registration between computed tomography (CT) and magnetic resonance (MR) images is associated with systematic uncertainties and the magnitude of these uncertainties is not well documented. The purpose of this study was to investigate the potential uncertainty of gold fiducial marker (GFM) registration for localized prostate cancer and to estimate the inter-observer bias in a clinical setting.
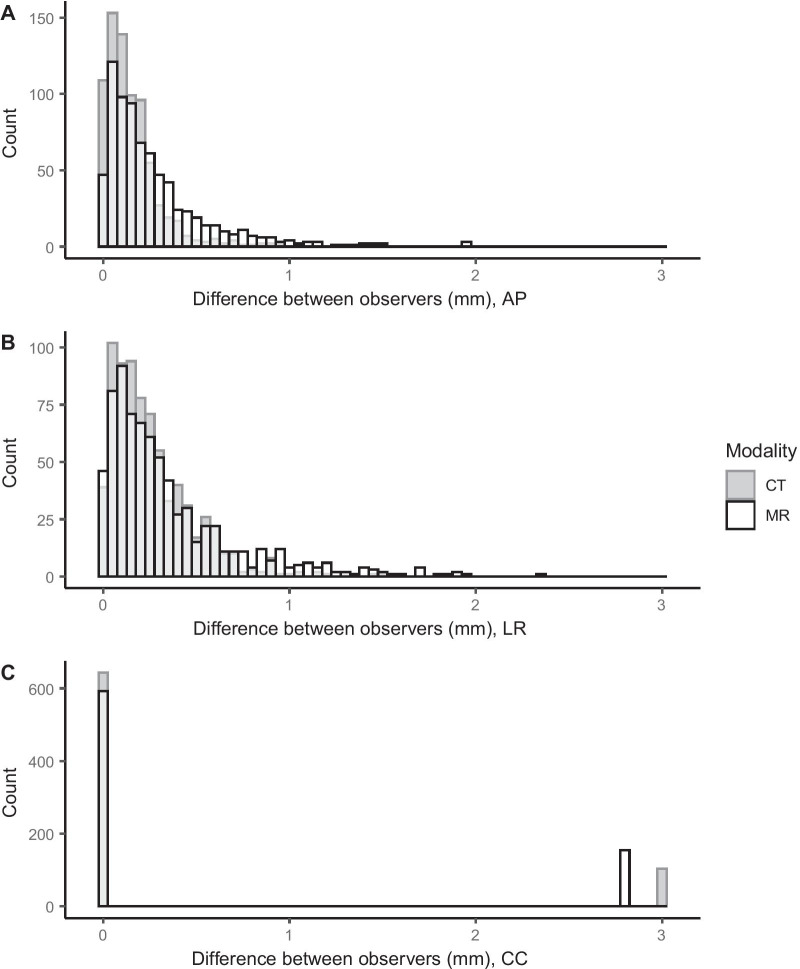
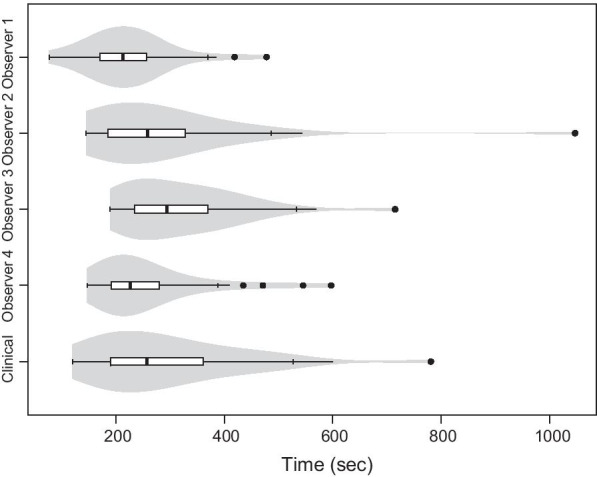
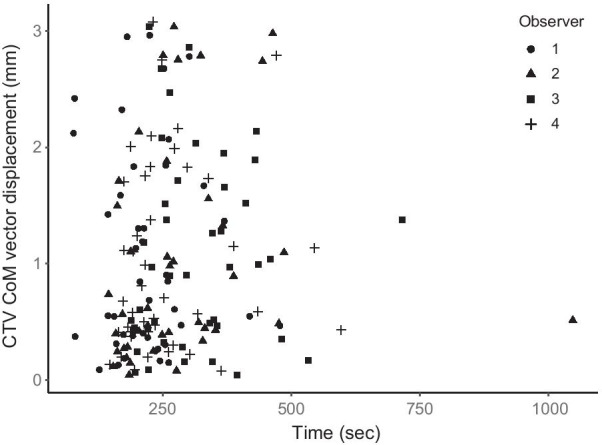
Methods: Four experienced observers registered CT and MR images for 42 prostate cancer patients. Manual GFM identification was followed by a landmark-based registration. The absolute difference between observers in GFM identification and the displacement of the clinical target volume (CTV) was investigated. The CTV center of mass (CoM) vector displacements, DICE-index and Hausdorff distances for the observer registrations were compared against a clinical baseline registration. The time allocated for the manual registrations was compared.
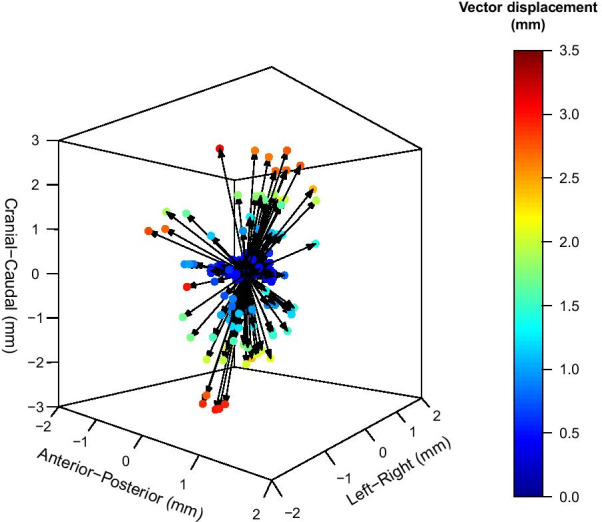
Results: Absolute difference in GFM identification between observers ranged from 0.0 to 3.0 mm. The maximum CTV CoM displacement from the clinical baseline was 3.1 mm. Displacements larger than or equal to 1 mm, 2 mm and 3 mm were 46%, 18% and 4%, respectively. No statistically significant difference was detected between observers in terms of CTV displacement. Median DICE-index and Hausdorff distance for the CTV, with their respective ranges were 0.94 [0.70-1.00] and 2.5 mm [0.7-8.7].
Conclusions: Registration of CT and MR images using GFMs for localized prostate cancer patients was subject to inter-observer bias on an individual patient level. A CTV displacement as large as 3 mm occurred for individual patients. These results show that GFM registration in a clinical setting is associated with uncertainties, which motivates the removal of inter-modality registrations in the radiotherapy workflow and a transition to an MRI-only workflow for localized prostate cancer.
Keywords: Computed tomography; Fiducial marker; Image registration; Inter-observer; Magnetic resonance imaging; Prostate cancer; Registration uncertainty.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Salembier C, Villeirs G, De Bari B, Hoskin P, Pieters BR, Van Vulpen M, et al. ESTRO ACROP consensus guideline on CT- and MRI-based target volume delineation for primary radiation therapy of localized prostate cancer. Radiother Oncol. 2018;127(1):49–61. doi: 10.1016/j.radonc.2018.01.014. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
