

Patient-ventilator asynchrony, impact on clinical outcomes and effectiveness of interventions: a systematic review and meta-analysis
- PMID: 34399855
- PMCID: PMC8365272
- DOI: 10.1186/s40560-021-00565-5
Patient-ventilator asynchrony, impact on clinical outcomes and effectiveness of interventions: a systematic review and meta-analysis
Abstract
Background: Patient-ventilator asynchrony (PVA) is a common problem in patients undergoing invasive mechanical ventilation (MV) in the intensive care unit (ICU), and may accelerate lung injury and diaphragm mis-contraction. The impact of PVA on clinical outcomes has not been systematically evaluated. Effective interventions (except for closed-loop ventilation) for reducing PVA are not well established.
Methods: We performed a systematic review and meta-analysis to investigate the impact of PVA on clinical outcomes in patients undergoing MV (Part A) and the effectiveness of interventions for patients undergoing MV except for closed-loop ventilation (Part B). We searched the Cochrane Central Register of Controlled Trials, MEDLINE, EMBASE, ClinicalTrials.gov, and WHO-ICTRP until August 2020. In Part A, we defined asynchrony index (AI) ≥ 10 or ineffective triggering index (ITI) ≥ 10 as high PVA. We compared patients having high PVA with those having low PVA.
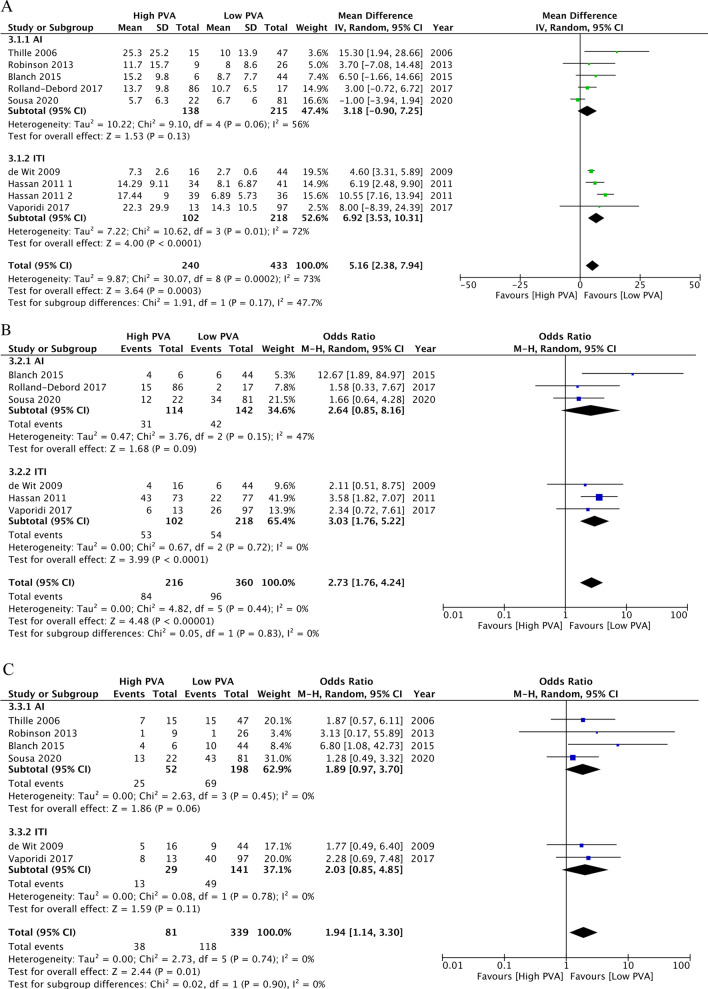
Results: Eight studies in Part A and eight trials in Part B fulfilled the eligibility criteria. In Part A, five studies were related to the AI and three studies were related to the ITI. High PVA may be associated with longer duration of mechanical ventilation (mean difference, 5.16 days; 95% confidence interval [CI], 2.38 to 7.94; n = 8; certainty of evidence [CoE], low), higher ICU mortality (odds ratio [OR], 2.73; 95% CI 1.76 to 4.24; n = 6; CoE, low), and higher hospital mortality (OR, 1.94; 95% CI 1.14 to 3.30; n = 5; CoE, low). In Part B, interventions involving MV mode, tidal volume, and pressure-support level were associated with reduced PVA. Sedation protocol, sedation depth, and sedation with dexmedetomidine rather than propofol were also associated with reduced PVA.
Conclusions: PVA may be associated with longer MV duration, higher ICU mortality, and higher hospital mortality. Physicians may consider monitoring PVA and adjusting ventilator settings and sedatives to reduce PVA. Further studies with adjustment for confounding factors are warranted to determine the impact of PVA on clinical outcomes. Trial registration protocols.io (URL: https://www.protocols.io/view/the-impact-of-patient-ventilator-asynchrony-in-adu-bsqtndwn , 08/27/2020).
Keywords: Asynchrony index; ICU; Ineffective triggering; Mechanical ventilation; Mortality; Patient–ventilator interaction.
© 2021. The Author(s).
Conflict of interest statement
None.
Figures


Similar articles
-
Effectiveness of dexmedetomidine versus propofol on extubation times, length of stay and mortality rates in adult cardiac surgery patients: a systematic review and meta-analysis.JBI Database System Rev Implement Rep. 2018 May;16(5):1220-1239. doi: 10.11124/JBISRIR-2017-003488. JBI Database System Rev Implement Rep. 2018. PMID: 29762314
-
Neurally Adjusted Ventilatory Assist vs. Conventional Mechanical Ventilation in Adults and Children With Acute Respiratory Failure: A Systematic Review and Meta-Analysis.Front Med (Lausanne). 2022 Feb 22;9:814245. doi: 10.3389/fmed.2022.814245. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35273975 Free PMC article.
-
Effect of Neurally Adjusted Ventilatory Assist on Patient-Ventilator Interaction in Mechanically Ventilated Adults: A Systematic Review and Meta-Analysis.Crit Care Med. 2019 Jul;47(7):e602-e609. doi: 10.1097/CCM.0000000000003719. Crit Care Med. 2019. PMID: 30882481
-
Patient-ventilator asynchrony in acute brain-injured patients: a prospective observational study.Ann Intensive Care. 2020 Oct 19;10(1):144. doi: 10.1186/s13613-020-00763-8. Ann Intensive Care. 2020. PMID: 33074406 Free PMC article.
-
Ineffective triggering predicts increased duration of mechanical ventilation.Crit Care Med. 2009 Oct;37(10):2740-5. doi: 10.1097/ccm.0b013e3181a98a05. Crit Care Med. 2009. PMID: 19886000
Cited by
-
Modern Sedation and Analgesia Strategies in Neurocritical Care.Curr Neurol Neurosci Rep. 2023 Apr;23(4):149-158. doi: 10.1007/s11910-023-01261-7. Epub 2023 Mar 7. Curr Neurol Neurosci Rep. 2023. PMID: 36881257 Review.
-
What is new in respiratory monitoring?J Clin Monit Comput. 2022 Jun;36(3):599-607. doi: 10.1007/s10877-022-00876-4. Epub 2022 May 13. J Clin Monit Comput. 2022. PMID: 35552970 Free PMC article. Review.
-
Specific Training Improves the Detection and Management of Patient-Ventilator Asynchrony.Respir Care. 2024 Jan 24;69(2):166-175. doi: 10.4187/respcare.11329. Respir Care. 2024. PMID: 38267230 Free PMC article.
-
Ability to identify patient-ventilator asynchronies in intensive care unit professionals: A multicenter cross-sectional analytical study.J Crit Care Med (Targu Mures). 2025 Apr 30;11(2):157-163. doi: 10.2478/jccm-2025-0017. eCollection 2025 Apr. J Crit Care Med (Targu Mures). 2025. PMID: 40386701 Free PMC article.
-
Patient Self-Inflicted Lung Injury-A Narrative Review of Pathophysiology, Early Recognition, and Management Options.J Pers Med. 2023 Mar 28;13(4):593. doi: 10.3390/jpm13040593. J Pers Med. 2023. PMID: 37108979 Free PMC article. Review.
References
-
- Gea J, Zhu E, Galdiz JB, Comtois N, Salazkin I, Fiz JA, et al. Functional consequences of eccentric contractions of the diaphragm. Archivos de bronconeumologia. 2009;45:68–74. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
