

IgG1 pan-neurofascin antibodies identify a severe yet treatable neuropathy with a high mortality
- PMID: 34400540
- PMCID: PMC8458075
- DOI: 10.1136/jnnp-2021-326343
IgG1 pan-neurofascin antibodies identify a severe yet treatable neuropathy with a high mortality
Abstract
Objectives: We aimed to define the clinical and serological characteristics of pan-neurofascin antibody-positive patients.
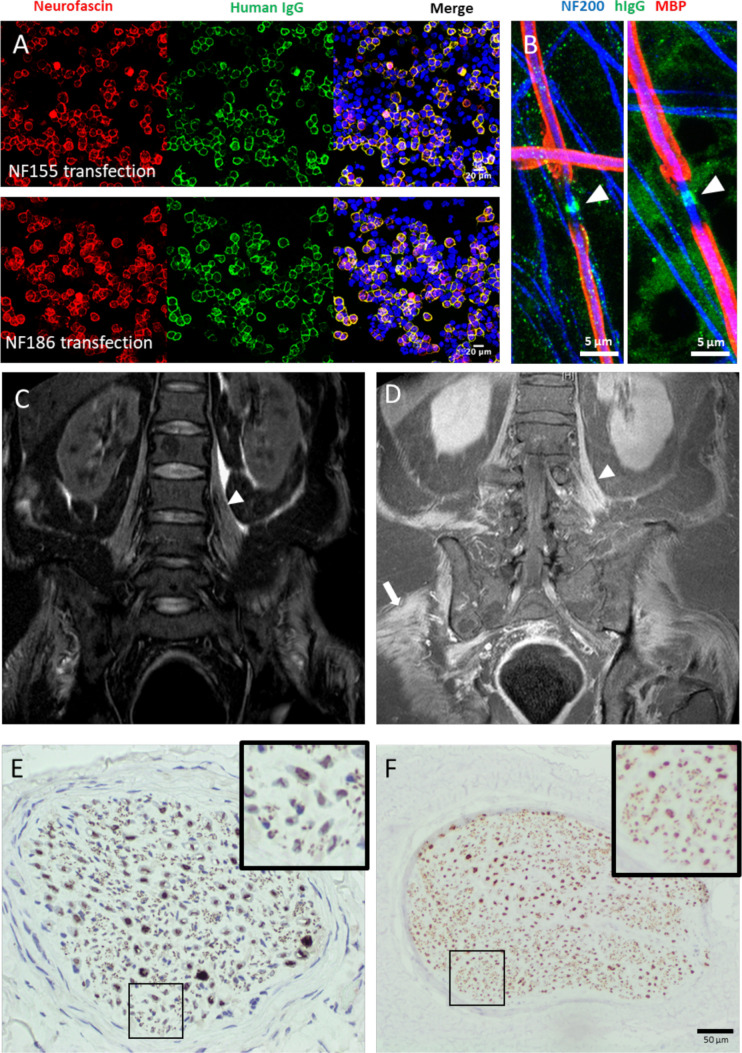
Methods: We tested serum from patients with suspected immune-mediated neuropathies for antibodies directed against nodal/paranodal protein antigens using a live cell-based assay and solid-phase platform. The clinical and serological characteristics of antibody-positive and seronegative patients were then compared. Sera positive for pan-neurofascin were also tested against live myelinated human stem cell-derived sensory neurons for antibody binding.
Results: Eight patients with IgG1-subclass antibodies directed against both isoforms of the nodal/paranodal cell adhesion molecule neurofascin were identified. All developed rapidly progressive tetraplegia. Cranial nerve deficits (100% vs 26%), autonomic dysfunction (75% vs 13%) and respiratory involvement (88% vs 14%) were more common than in seronegative patients. Four patients died despite treatment with one or more modalities of standard immunotherapy (intravenous immunoglobulin, steroids and/or plasmapheresis), whereas the four patients who later went on to receive the B cell-depleting therapy rituximab then began to show progressive functional improvements within weeks, became seronegative and ultimately became functionally independent.
Conclusions: IgG1 pan-neurofascin antibodies define a very severe autoimmune neuropathy. We urgently recommend trials of targeted immunotherapy for this serologically classified patient group.
Keywords: neuroimmunology; neuropathy.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: JF has received research grants from the Guarantors of Brain and GBS|CIDP Foundation International. TL has received speaker’s honoraria from CSL Behring and Akcea. AJD, JW, RK, AMR, TM, ND, RR, DB and GL report no disclosures or conflicts of interest. SR has received speaker’s honoraria from Fresenius, Alnylam and Excemed, and payments to provide expert medicolegal advice on inflammatory neuropathies and their treatment. He has received complimentary registration and prize money from the Peripheral Nerve Society, and a travel bursary from the European School of Neuroimmunology. He is a member of the GBS and Associated Inflammatory Neuropathies (GAIN) patient charity medical advisory board. He runs a not-for-profit nodal/paranodal antibody testing service at the Nuffield Department of Clinical Neurosciences, John Radcliffe Hospital, Oxford, UK, in partnership with Clinical Laboratory Immunology of Oxford University Hospitals.
Figures
Comment in
-
Autoimmune nodopathies: treatable neuropathies beyond traditional classifications.J Neurol Neurosurg Psychiatry. 2021 Oct;92(10):1025. doi: 10.1136/jnnp-2021-326676. Epub 2021 Aug 16. J Neurol Neurosurg Psychiatry. 2021. PMID: 34400541 No abstract available.
References
-
- Joint Task Force of the EFNS and the PNS . European Federation of Neurological Societies/Peripheral Nerve Society Guideline on management of chronic inflammatory demyelinating polyradiculoneuropathy: Report of a joint task force of the European Federation of Neurological Societies and the Peripheral Nerve Society - First Revision. J Peripher Nerv Syst JPNS 2010;15:1–9. 10.1111/j.1529-8027.2010.00245.x - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical