

Miliary brain tuberculosis in an infant
- PMID: 34401018
- PMCID: PMC8350015
- DOI: 10.1016/j.radcr.2021.07.005
Miliary brain tuberculosis in an infant
Abstract
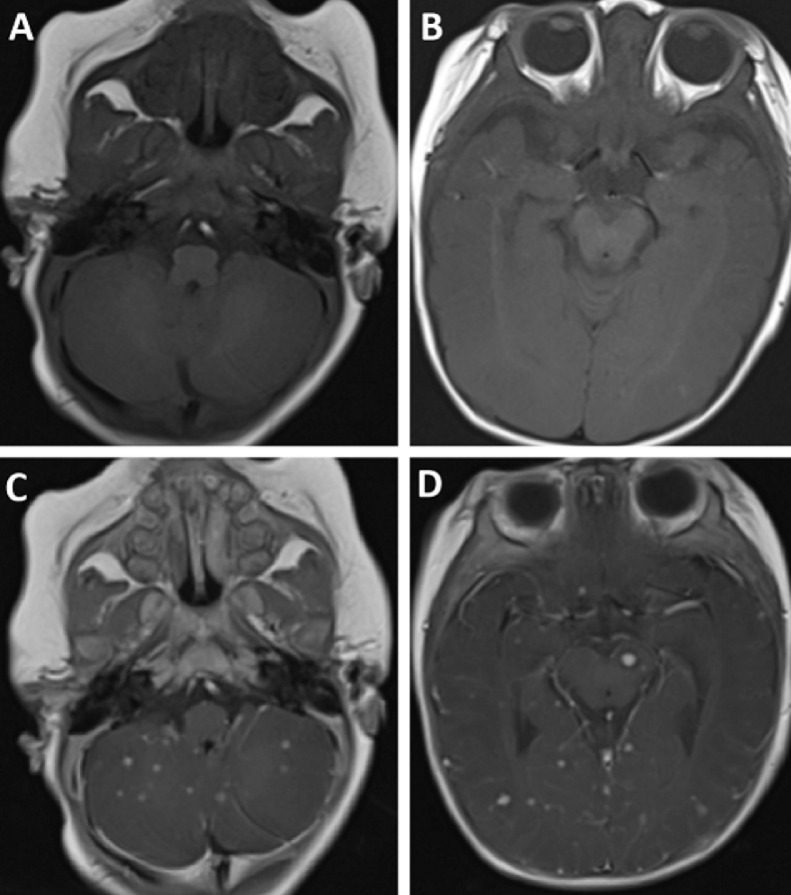
Tuberculosis remains prevalent in developing countries. Central nervous system tuberculosis often occurs secondary to pulmonary tuberculosis, transmitted through the bloodstream, and has a high mortality rate. Meningitis is the most common presentation of central nervous system tuberculosis, followed by tuberculoma, tuberculous brain abscess, and miliary tuberculosis. In this report, we present a case of miliary tuberculosis in a 3 month-old boy. The patient had a fever and was breathless for 1 month. The patient appeared cyanotic, experienced a seizure, and became comatose. Chest computed tomography scan suggested a pulmonary miliary tuberculosis abscess in the right lung and mediastinal lymph node tuberculosis. Brain magnetic resonance imaging showed the lesions were homogeneously enhancing tiny 2-3 mm nodules characteristic of miliary TB. Polymerase chain reaction of the cerebrospinal fluid and sputum samples confirmed tuberculosis. The patient died 1 month after diagnosis.
Keywords: Brain tuberculosis; Central nervous system; Children; Miliary tuberculosis.
© 2021 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures


References
Publication types
LinkOut - more resources
Full Text Sources
