

doi: 10.1016/j.eats.2021.04.021.
eCollection 2021 Aug.
All-Inside Repair for Radial Tear at the Posterior Horn of the Lateral Meniscus: A Figure-8 Suture Technique
Affiliations
- PMID: 34401242
- PMCID: PMC8355411
- DOI: 10.1016/j.eats.2021.04.021
Item in Clipboard
All-Inside Repair for Radial Tear at the Posterior Horn of the Lateral Meniscus: A Figure-8 Suture Technique
Arthrosc Tech.
.
Abstract
Arthroscopic suture repair for a radial tear at the posterior horn of the lateral meniscus poses a technical procedure for surgeons. We describe an all-inside repair technique using all-inside meniscal repair devices without adding any accessory portals. This simple technique provides precise reduction and stabilization of the meniscus by pinching 2 all-inside vertical sutures consecutively across the tear site.
© 2021 by the Arthroscopy Association of North America. Published by Elsevier.
Figures
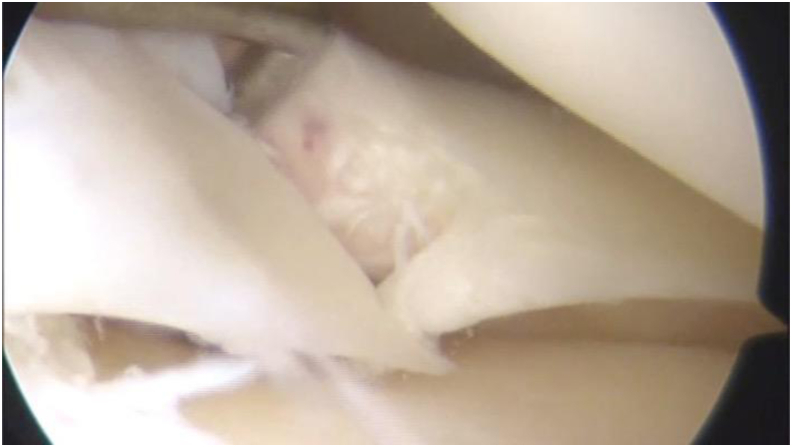
A radial tear at the posterior horn of the lateral meniscus in left knee. This type of tear is usually accompanied by the anterior cruciate ligament injury.
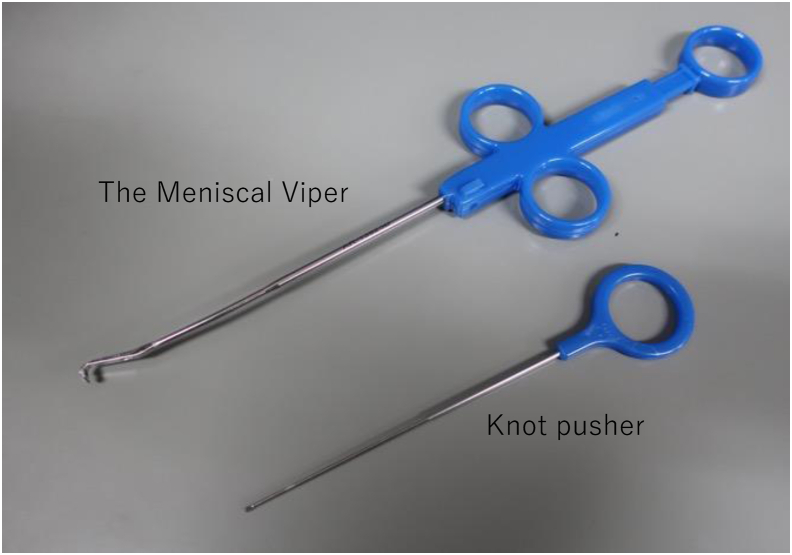
The Meniscal Viper Kit is an all-inside passing sutures system, repairing for the posterior segment of the meniscus without needle passage through the capsule. This system fashions the all-inside vertical suture, which is well fit for repairing the longitudinal tears. In this report, the Viper is adapted for the radial tear of the lateral meniscus.
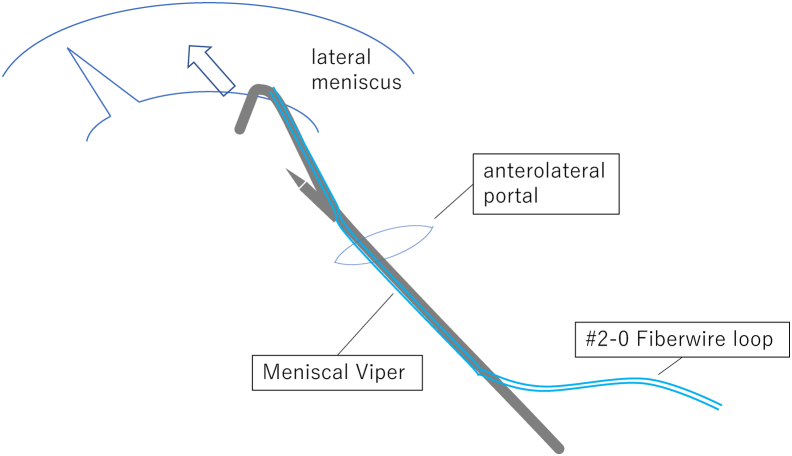
Insert the Meniscal Viper through anterolateral portal while inserting the arthroscope from the anteromedial as a viewing portal. The Viper is set with a looped no. 2-0 FiberWire. Although a cannula is not ordinarily required for use, it can be used to aid insertion of the Viper and avoid fat pad interference during the procedure.
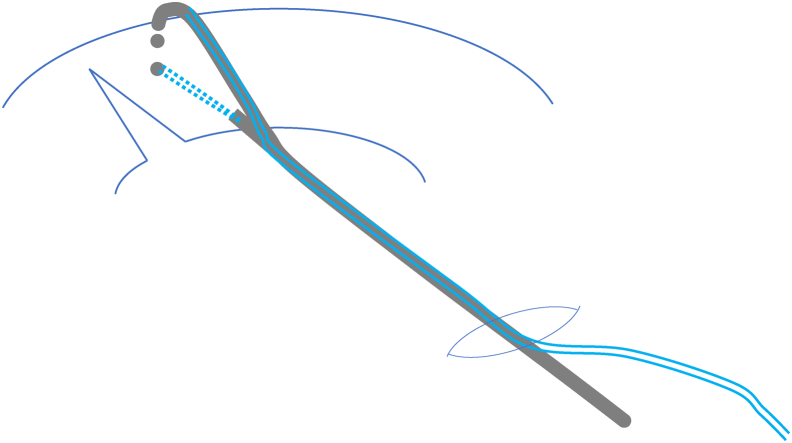
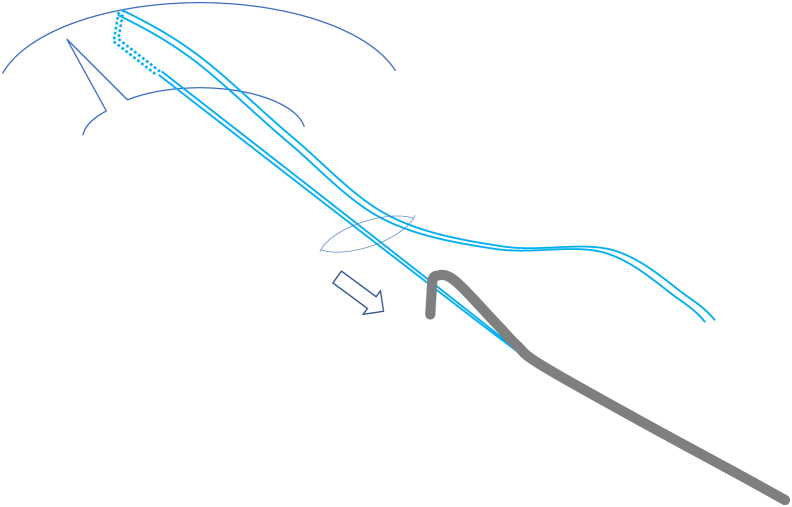
The tip of the Viper is inserted and rotated down into the position. The primary suture is positioned 5 to 10 mm apart from the tear site toward the middle segment side. The Viper hook is gripped along the meniscal outer rim, and the needle is inserted. The hook should hang deep, and the needle insertion should be near the anterior margin of the lateral meniscus to bundle the circumference fiber of the meniscus more. By pushing the needle toward the hook through the substantial meniscus, the needle tip captures the looped no. 2-0 FiberWire.
The needle retrieves the suture loop, and the Viper is extracted from the joint.
The Viper system is set with the same loop suture again.
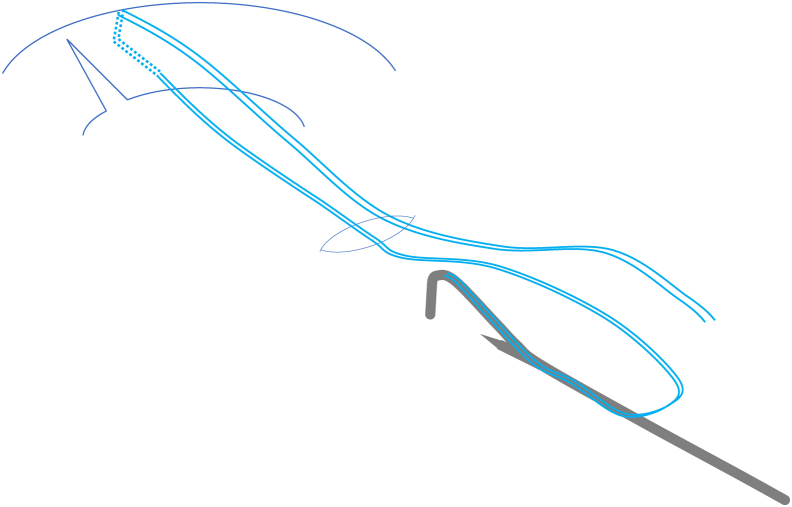
The second suture refrains the same vertical stitch as the primary one at the other side of the posterior horn of the radial lateral meniscus tear. The tip of the Viper’s hook is positioned near the tibial insertion of the posterior cruciate ligament. The needle tip of the second suture captures the looped no. 2-0 FiberWire again.
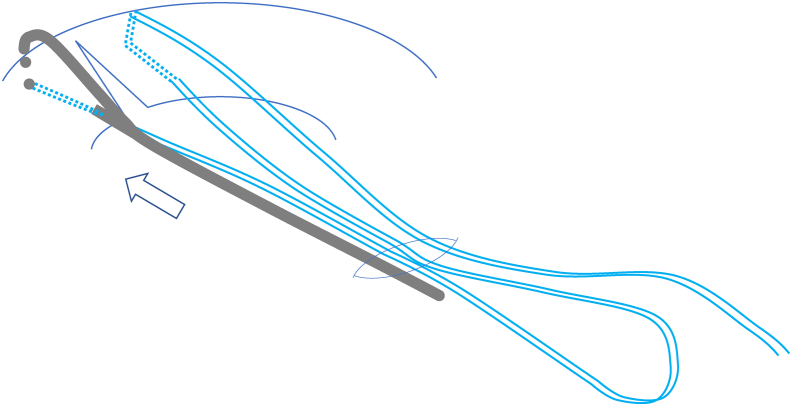
The Viper needle retrieves the suture loop, and the viper, with the looped suture end, is extracted out through the anterolateral portal. A consecutive vertical suture at the site of the radial tear is confirmed.
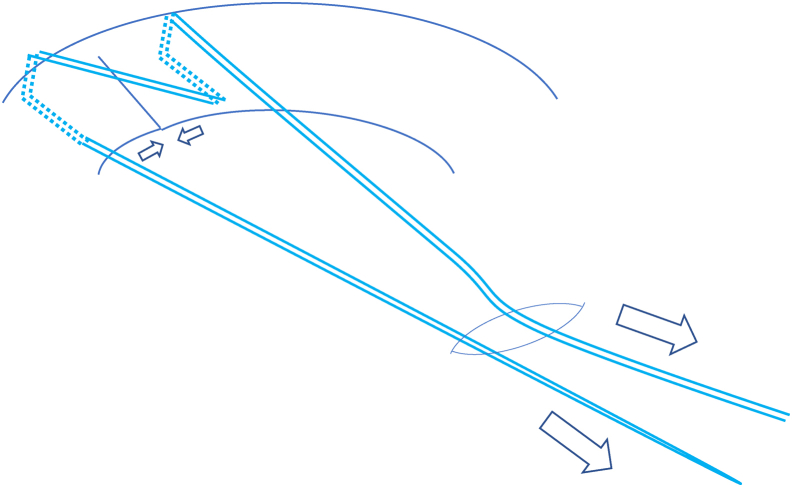
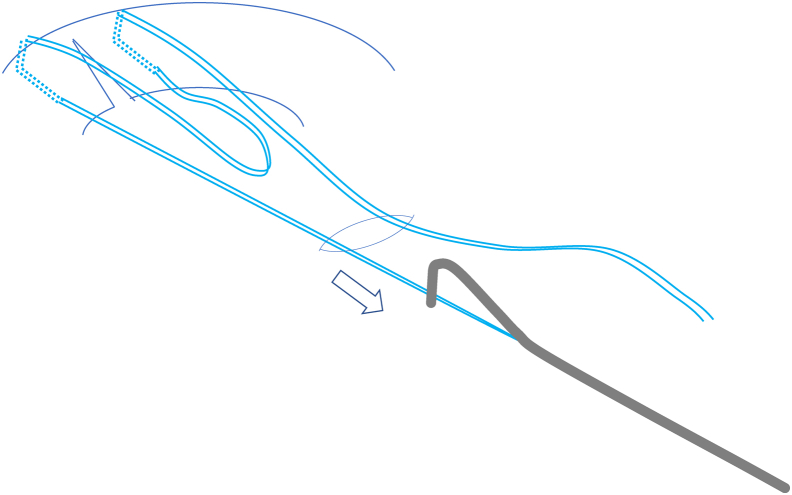
By pulling the 2 suture ends simultaneously little by little, the tear in the meniscus is reduced. An oblique running thread on the tear site is observed.
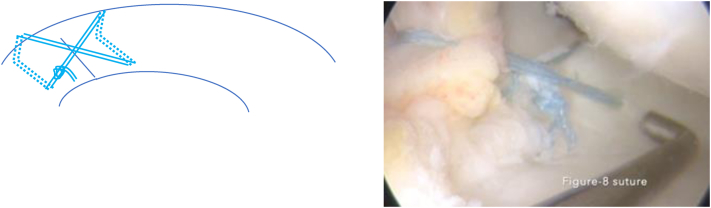
The suture is tied by drawing a single modified racking hitch to the meniscus, followed by a couple of half hitches to secure the knot. After the remaining no. 2-0 FiberWire is cut with the suture cutter, a figure-8 suture is run across the femoral surface and vertically through the mid-substance beside the tear site of the meniscus.
References
-
- Markes A.R., Hodax J.D., Ma C.B. Meniscus form and function. Clin Sports Med. 2020;39:1–12. - PubMed
-
- Mao D.W., Upadhyay U., Thalanki S., Lee D.Y.H. All-inside lateral meniscal repair via anterolateral portal increases risk of vascular injury: A cadaveric study. Arthroscopy. 2020;36:225–232. - PubMed
-
- Song H.S., Bae T.Y., Park B.Y., Shim J., In Y. Repair of a radial tear in the posterior horn of the lateral meniscus. Knee. 2014;21:1185–1190. - PubMed
LinkOut - more resources
Full Text Sources
