

Delirium in critical illness: clinical manifestations, outcomes, and management
- PMID: 34401939
- PMCID: PMC8366492
- DOI: 10.1007/s00134-021-06503-1
Delirium in critical illness: clinical manifestations, outcomes, and management
Abstract
Delirium is the most common manifestation of brain dysfunction in critically ill patients. In the intensive care unit (ICU), duration of delirium is independently predictive of excess death, length of stay, cost of care, and acquired dementia. There are numerous neurotransmitter/functional and/or injury-causing hypotheses rather than a unifying mechanism for delirium. Without using a validated delirium instrument, delirium can be misdiagnosed (under, but also overdiagnosed and trivialized), supporting the recommendation to use a monitoring instrument routinely. The best-validated ICU bedside instruments are CAM-ICU and ICDSC, both of which also detect subsyndromal delirium. Both tools have some inherent limitations in the neurologically injured patients, yet still provide valuable information about delirium once the sequelae of the primary injury settle into a new post-injury baseline. Now it is known that antipsychotics and other psychoactive medications do not reliably improve brain function in critically ill delirious patients. ICU teams should systematically screen for predisposing and precipitating factors. These include exacerbations of cardiac/respiratory failure or sepsis, metabolic disturbances (hypoglycemia, dysnatremia, uremia and ammonemia) receipt of psychoactive medications, and sensory deprivation through prolonged immobilization, uncorrected vision and hearing deficits, poor sleep hygiene, and isolation from loved ones so common during COVID-19 pandemic. The ABCDEF (A2F) bundle is a means to facilitate implementation of the 2018 Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU (PADIS) Guidelines. In over 25,000 patients across nearly 100 institutions, the A2F bundle has been shown in a dose-response fashion (i.e., greater bundle compliance) to yield improved survival, length of stay, coma and delirium duration, cost, and less ICU bounce-backs and discharge to nursing homes.
Keywords: Antipsychotics; Cognitive impairment; Critical care; Delirium; ICU Liberation.
© 2021. Springer-Verlag GmbH Germany, part of Springer Nature.
Figures
References
-
- Morandi A, Piva S, Ely EW, Myatra SN, Salluh JIF, Amare D, Azoulay E, Bellelli G, Csomos A, Fan E, et al. Worldwide survey of the "assessing pain, both spontaneous awakening and breathing trials, choice of drugs, delirium monitoring/management, early exercise/mobility, and family empowerment" (ABCDEF) bundle. Crit Care Med. 2017;45(11):e1111–e1122. doi: 10.1097/CCM.0000000000002640. - DOI - PMC - PubMed
-
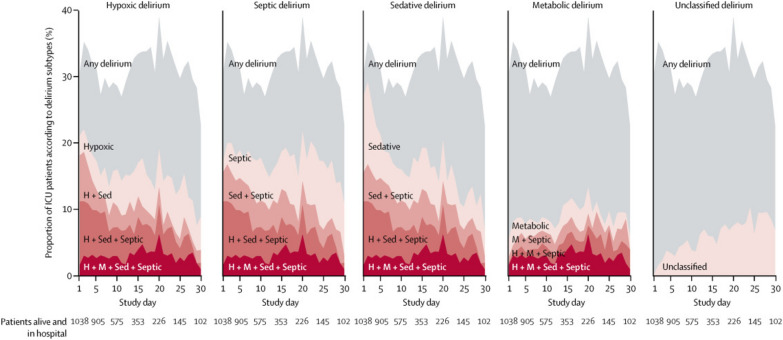
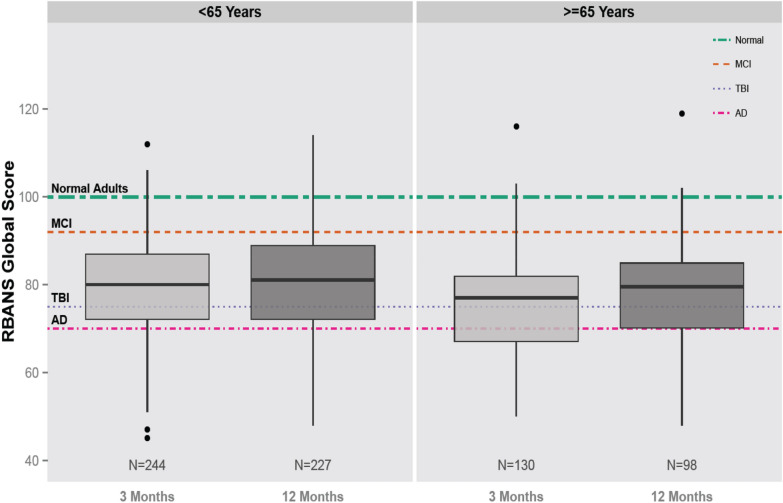
- Girard TD, Thompson JL, Pandharipande PP, Brummel NE, Jackson JC, Patel MB, Hughes CG, Chandrasekhar R, Pun BT, Boehm LM, et al. Clinical phenotypes of delirium during critical illness and severity of subsequent long-term cognitive impairment: a prospective cohort study. Lancet Respir Med. 2018;6(3):213–222. doi: 10.1016/S2213-2600(18)30062-6. - DOI - PMC - PubMed
-
- Chanques G, Ely EW, Garnier O, Perrigault F, Eloi A, Carr J, Rowan CM, Prades A, de Jong A, Moritz-Gasser S, et al. The 2014 updated version of the confusion assessment method for the intensive care unit compared to the 5th version of the diagnostic and statistical manual of mental disorders and other current methods used by intensivists. Ann Intensive Care. 2018;8(1):33. doi: 10.1186/s13613-018-0377-7. - DOI - PMC - PubMed
-
- American Psychiatric Association . Diagnostic and statistical manual of mental disorders: DSM-5. American Psychiatric Association; 2013.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
