

Association of Race and Ethnicity and Medicare Program Type With Ambulatory Care Access and Quality Measures
- PMID: 34402828
- PMCID: PMC8371568
- DOI: 10.1001/jama.2021.10413
Association of Race and Ethnicity and Medicare Program Type With Ambulatory Care Access and Quality Measures
Abstract
Importance: There are racial inequities in health care access and quality in the United States. It is unknown whether such differences for racial and ethnic minority beneficiaries differ between Medicare Advantage and traditional Medicare or whether access and quality are better for minority beneficiaries in 1 of the 2 programs.
Objective: To compare differences in rates of enrollment, ambulatory care access, and ambulatory care quality by race and ethnicity in Medicare Advantage vs traditional Medicare.
Design, setting, and participants: Exploratory observational cohort study of a nationally representative sample of 45 833 person-years (26 887 persons) in the Medicare Current Beneficiary Survey from 2015 to 2018, comparing differences in program enrollment and measures of access and quality by race and ethnicity.
Exposures: Minority race and ethnicity (Black, Hispanic, Native American, or Asian/Pacific Islander) vs White or multiracial; Medicare Advantage vs traditional Medicare enrollment.
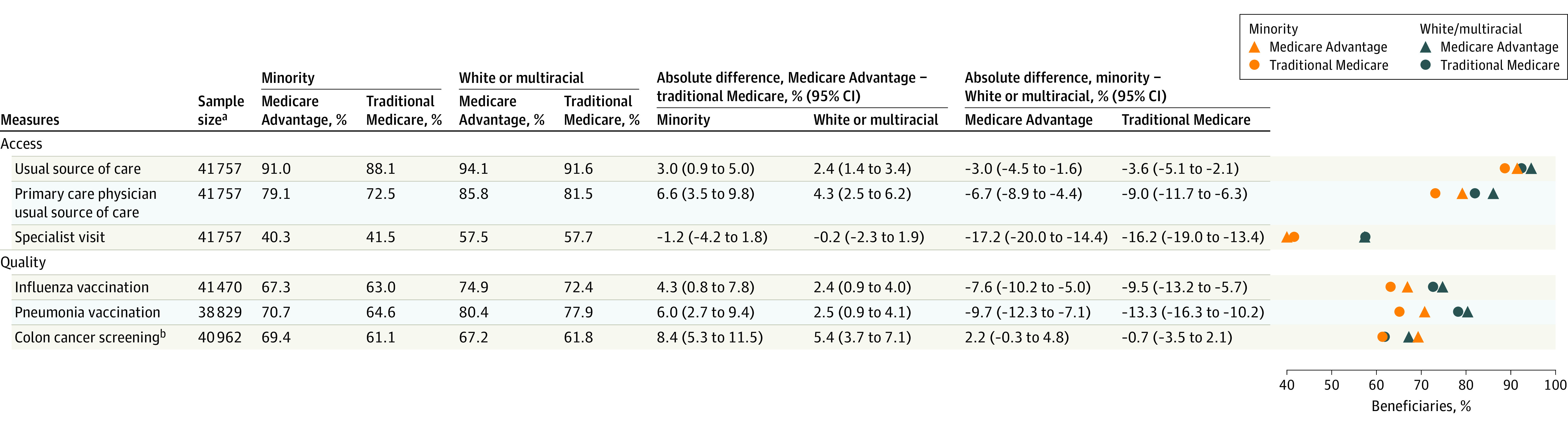
Main outcomes and measures: Six patient-reported measures of ambulatory care access (whether a beneficiary had a usual source of care in the past year, had a primary care clinician usual source of care, or had a specialist visit) and quality (influenza vaccination, pneumonia vaccination, and colon cancer screening).
Results: The final sample included 6023 persons (mean age, 68.9 [SD, 12.6] years; 57.3% women) from minority groups and 20 864 persons (mean age, 71.9 [SD, 10.8] years; 54.9% women) from White or multiracial groups, who accounted for 9816 and 36 017 person-years, respectively. Comparing Medicare Advantage vs traditional Medicare among minority beneficiaries, those in Medicare Advantage had significantly better rates of access to a primary care clinician usual source of care (79.1% vs 72.5%; adjusted marginal difference, 4.0%; 95% CI, 1.0%-6.9%), influenza vaccinations (67.3% vs 63.0%; adjusted marginal difference, 5.2%; 95% CI, 1.9%-8.5%), pneumonia vaccinations (70.7% vs 64.6%; adjusted marginal difference, 6.1%; 95% CI, 2.7%-9.4%), and colon cancer screenings (69.4% vs 61.1%; adjusted marginal difference, 7.1%; 95% CI, 3.8%-10.3%). Comparing minority vs White or multiracial beneficiaries across both programs, minority beneficiaries had significantly lower rates of access to a primary care clinician usual source of care (adjusted marginal difference, 4.7%; 95% CI, 2.5%-6.8%), specialist visits (adjusted marginal difference, 10.8%; 95% CI, 8.3%-13.3%), influenza vaccinations (adjusted marginal difference, 4.3%; 95% CI, 1.2%-7.4%), and pneumonia vaccinations (adjusted marginal difference, 6.4%; 95% CI, 3.9%-9.0%). The interaction of race and ethnicity with insurance type was not statistically significant for any of the 6 outcome measures.
Conclusions and relevance: In this exploratory study of Medicare beneficiaries in 2015-2018, enrollment in Medicare Advantage vs traditional Medicare was significantly associated with better outcomes for access and quality among minority beneficiaries; however, minority beneficiaries were significantly more likely to experience worse outcomes for most access and quality measures than White or multiracial beneficiaries in both programs.
Conflict of interest statement
Figures
Comment in
-
Ending Structural Racism in the US Health Care System to Eliminate Health Care Inequities.JAMA. 2021 Aug 17;326(7):613-615. doi: 10.1001/jama.2021.11160. JAMA. 2021. PMID: 34402851 No abstract available.
References
-
- Johnston KJ, Hockenberry JM. Are two heads better than one or do too many cooks spoil the broth? the trade-off between physician division of labor and patient continuity of care for older adults with complex chronic conditions. Health Serv Res. 2016;51(6):2176-2205. doi:10.1111/1475-6773.12600 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
