

Targeting residual inflammatory risk in coronary disease: to catch a monkey by its tail
- PMID: 34403066
- PMCID: PMC8724334
- DOI: 10.1007/s12471-021-01605-3
Targeting residual inflammatory risk in coronary disease: to catch a monkey by its tail
Abstract
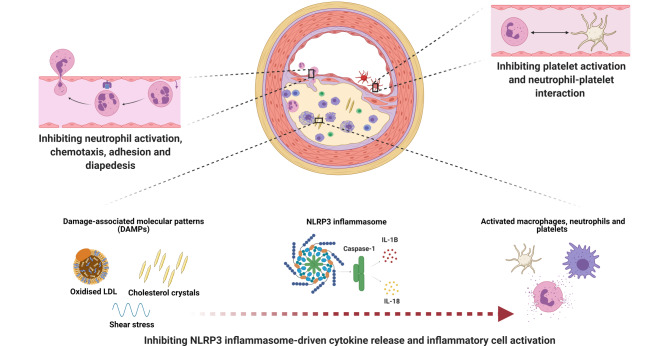
Patients with coronary disease remain at high risk for future cardiovascular events, even with optimal risk factor modification, lipid-lowering drugs and antithrombotic regimens. A myriad of inflammatory pathways contribute to progression of the atherosclerotic burden in these patients. Only in the last few years has the inflammatory biology of atherosclerosis translated into clinical therapeutic options. Low-dose colchicine can provide a clinically relevant reduction in the risk for composite and individual major cardiovascular outcomes in patients with acute and chronic coronary syndromes. Among others, its anti-inflammatory effects in atherosclerosis seem to be related to neutrophil recruitment and adhesion, inflammasome inhibition, and morphological changes in platelets and platelet aggregation. Future research is aimed at further elucidating its particular mechanism of action, as well as identifying patients with the highest expected benefit and evaluating efficacy in other vascular beds. These data will help to formulate the role of colchicine and other anti-inflammatory drugs in patients with coronary disease and atherosclerosis in general in the near future.
Keywords: Acute coronary syndrome; Atherosclerosis; Chronic coronary disease; Inflammation.
© 2021. The Author(s).
Conflict of interest statement
A.T.L. Fiolet, T.S.J. Opstal, M.J.M. Silvis, J.H. Cornel and A. Mosterd declare that they have no competing interests.
Figures
References
-
- Roth GA, Huffman MD, Moran AE, et al. Global and regional patterns in cardiovascular mortality from 1990 to 2013. Circulation. 2015;132:1667–1678. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
