

Best practices in pediatric sepsis: building and sustaining an evidence-based pediatric sepsis quality improvement program
- PMID: 34404310
- PMCID: PMC8891392
- DOI: 10.1080/21548331.2021.1966252
Best practices in pediatric sepsis: building and sustaining an evidence-based pediatric sepsis quality improvement program
Abstract
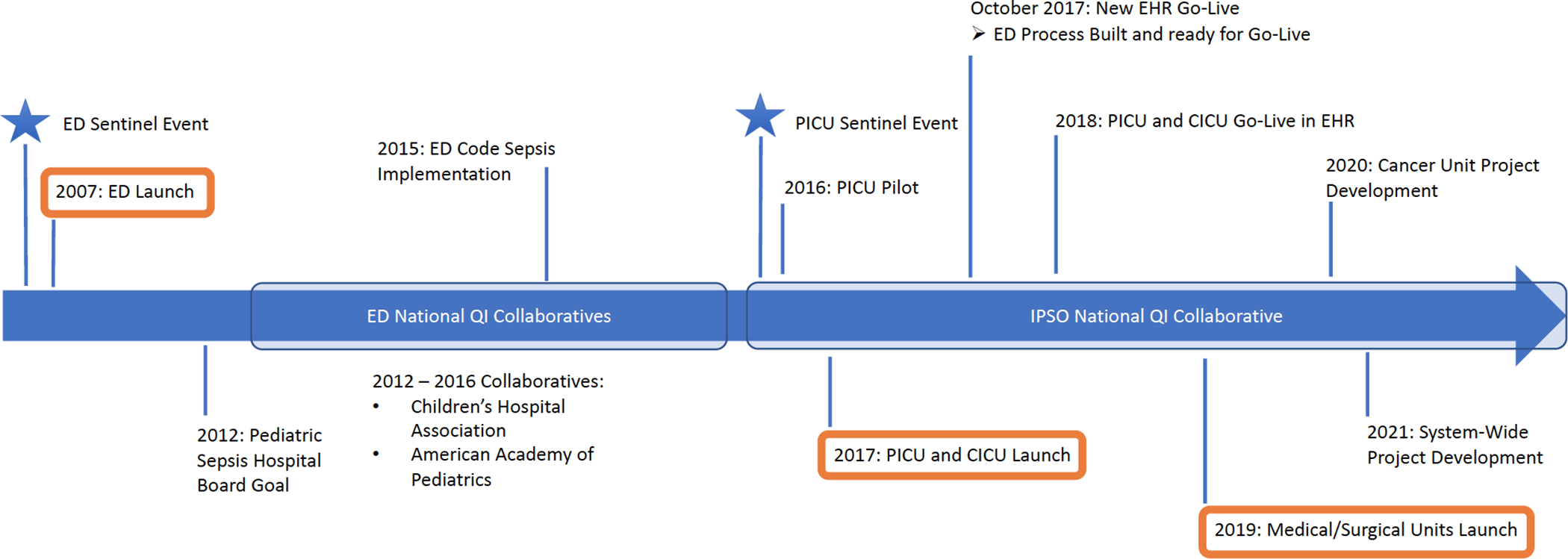
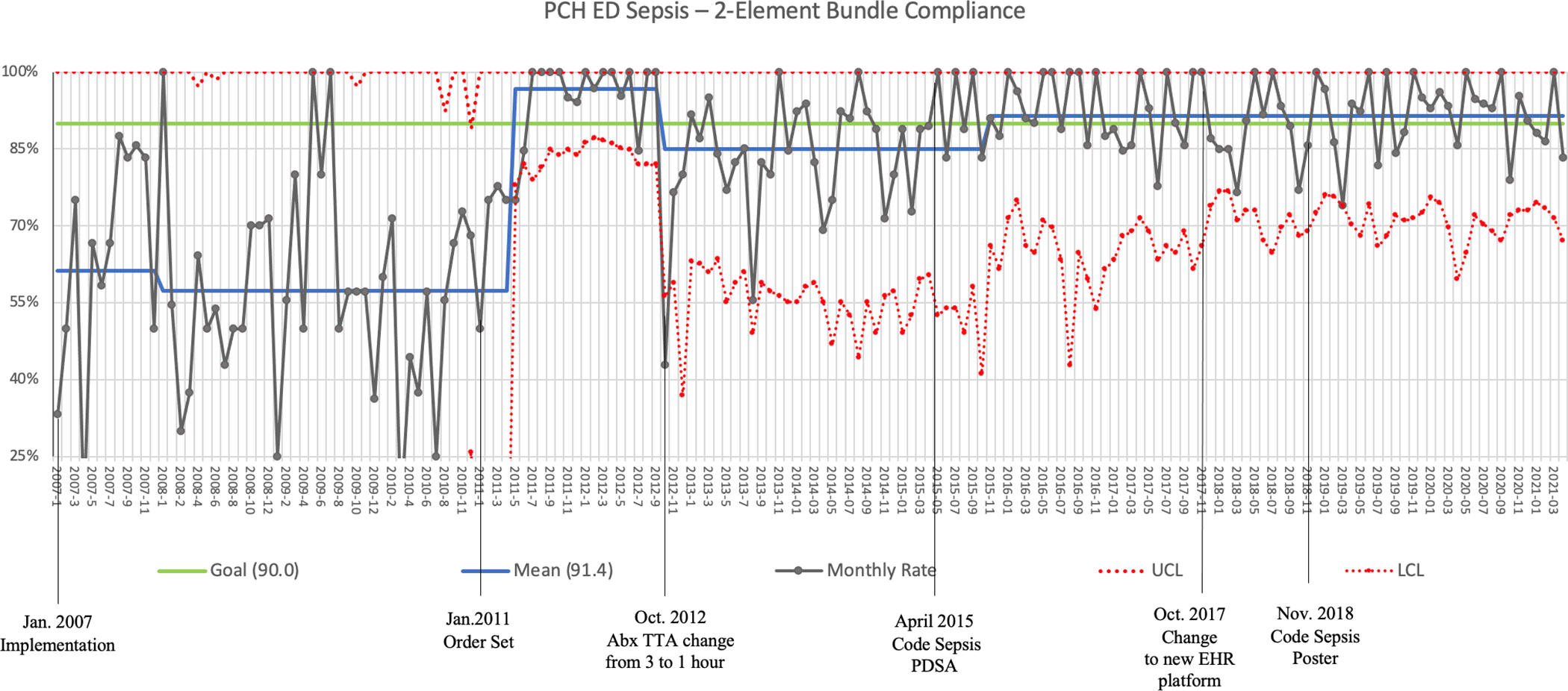
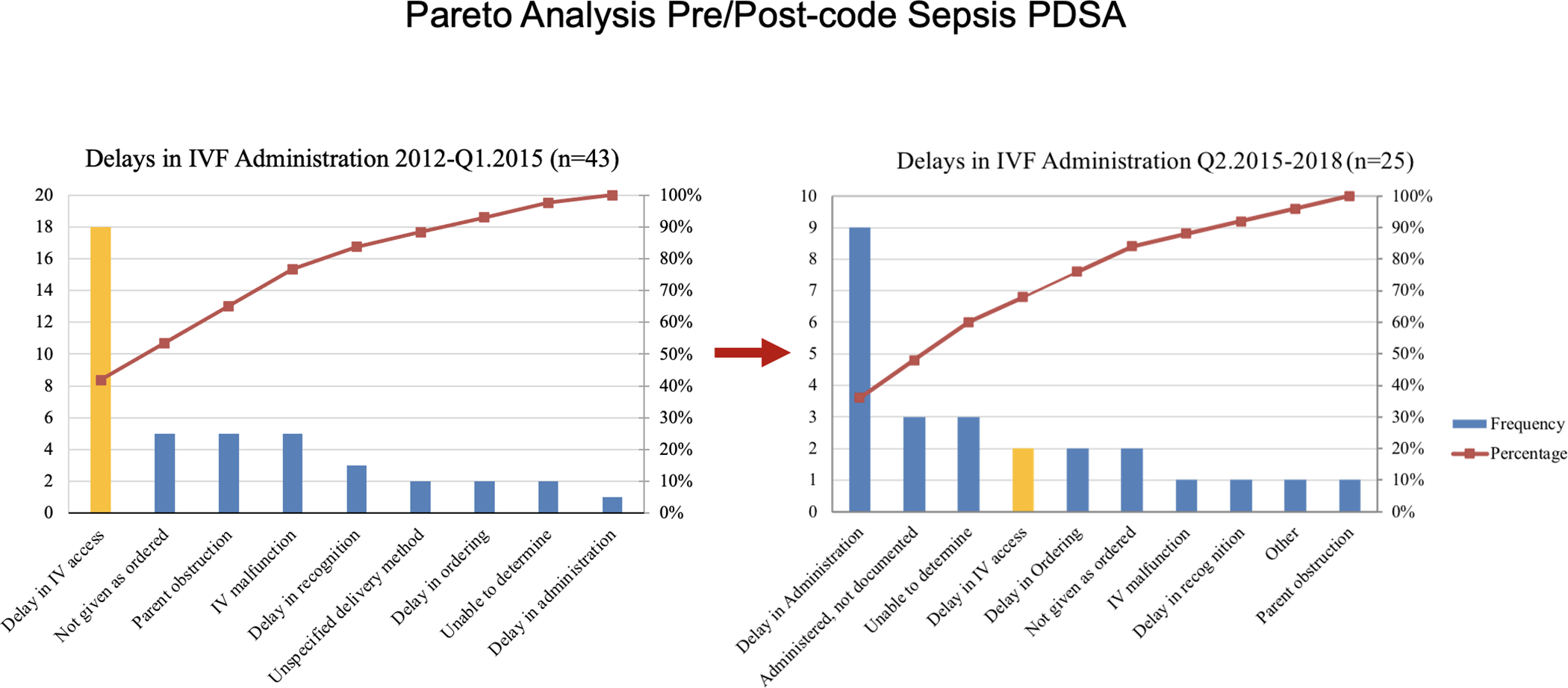
Pediatric sepsis is a common problem worldwide and is associated with significant morbidity and mortality. Best practice recommendations have been published by both the American College of Critical Care Medicine and the Surviving Sepsis Campaign to guide the recognition and treatment of pediatric sepsis. However, implementation of these recommendations can be challenging due to the complexity of the care required and intensity of resources needed to successfully implement programs. This paper outlines the experience with implementation of a pediatric sepsis quality improvement program at Primary Children's Hospital, a free-standing, quaternary care children's hospital in Salt Lake City. The hospital has implemented sepsis projects across multiple care settings. Challenges, lessons learned, and suggestions for implementation are described.PLAIN LANGUAGE SUMMARYSepsis is a life-threatening condition that results from an inappropriate response to an infection by the body's immune system. All children are potentially susceptible to sepsis, with nearly 8,000 children dying from the disease in the US each year. Sepsis is a complicated disease, and several international groups have published guidelines to help hospital teams treat children with sepsis appropriately. However, because recognizing and treating sepsis in children is challenging and takes a coordinated effort from many different types of healthcare team members, following the international sepsis guidelines effectively can be difficult and resource intensive. This paper describes how one children's hospital (Primary Children's Hospital in Salt Lake City, Utah) approached the challenge of implementing pediatric sepsis guidelines, some lessons learned from their experience, and suggestions for others interested in implementing sepsis guidelines for children.
Keywords: Pediatrics; guideline adherence; pediatric emergency medicine; quality improvement; sepsis; septic shock.
Figures
References
-
- Fleischmann-Struzek C, Goldfarb DM, Schlattmann P, et al. The global burden of paediatric and neonatal sepsis: a systematic review. Lancet Respir Med. 2018;6(3):223–230. - PubMed
-
- Weiss SL, Peters MJ, Alhazzani W, et al. Surviving Sepsis Campaign International Guidelines for the Management of Septic Shock and Sepsis-Associated Organ Dysfunction in Children. Pediatr Crit Care Med. 2020;21(2):e52–e106. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical