

Mucormycosis-induced upper gastrointestinal ulcer perforation in immunocompetent patients: a report of two cases
- PMID: 34404350
- PMCID: PMC8370051
- DOI: 10.1186/s12876-021-01881-8
Mucormycosis-induced upper gastrointestinal ulcer perforation in immunocompetent patients: a report of two cases
Abstract
Background: Gastrointestinal mucormycosis (GIM) is a rare, opportunistic fungal infection with poor prognosis. Clinically, it is difficult to diagnose GIM owing to its nonspecific clinical symptoms and poor suspicion. The estimated incidence of GIM is inaccurate, and most cases are diagnosed accidentally during surgery or upon postmortem examination. GIM usually occurs in patients with immune deficiencies or diabetes. Here, we report two cases of immunocompetent young patients with GIM who had good prognosis after treatment. Compared to other case reports on GIM, our cases had unusual infection sites and no obvious predisposing factors, which make it important to highlight these cases.
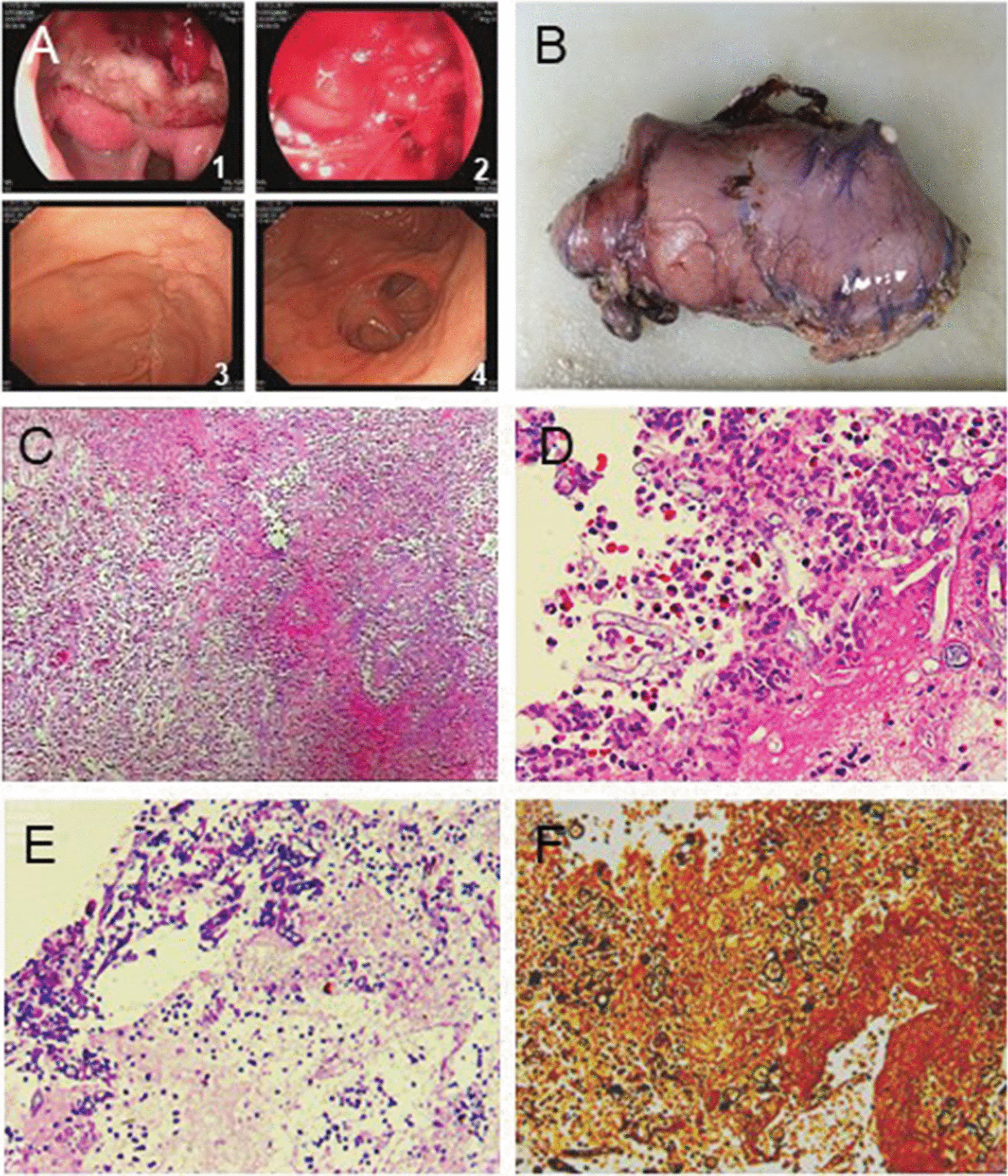
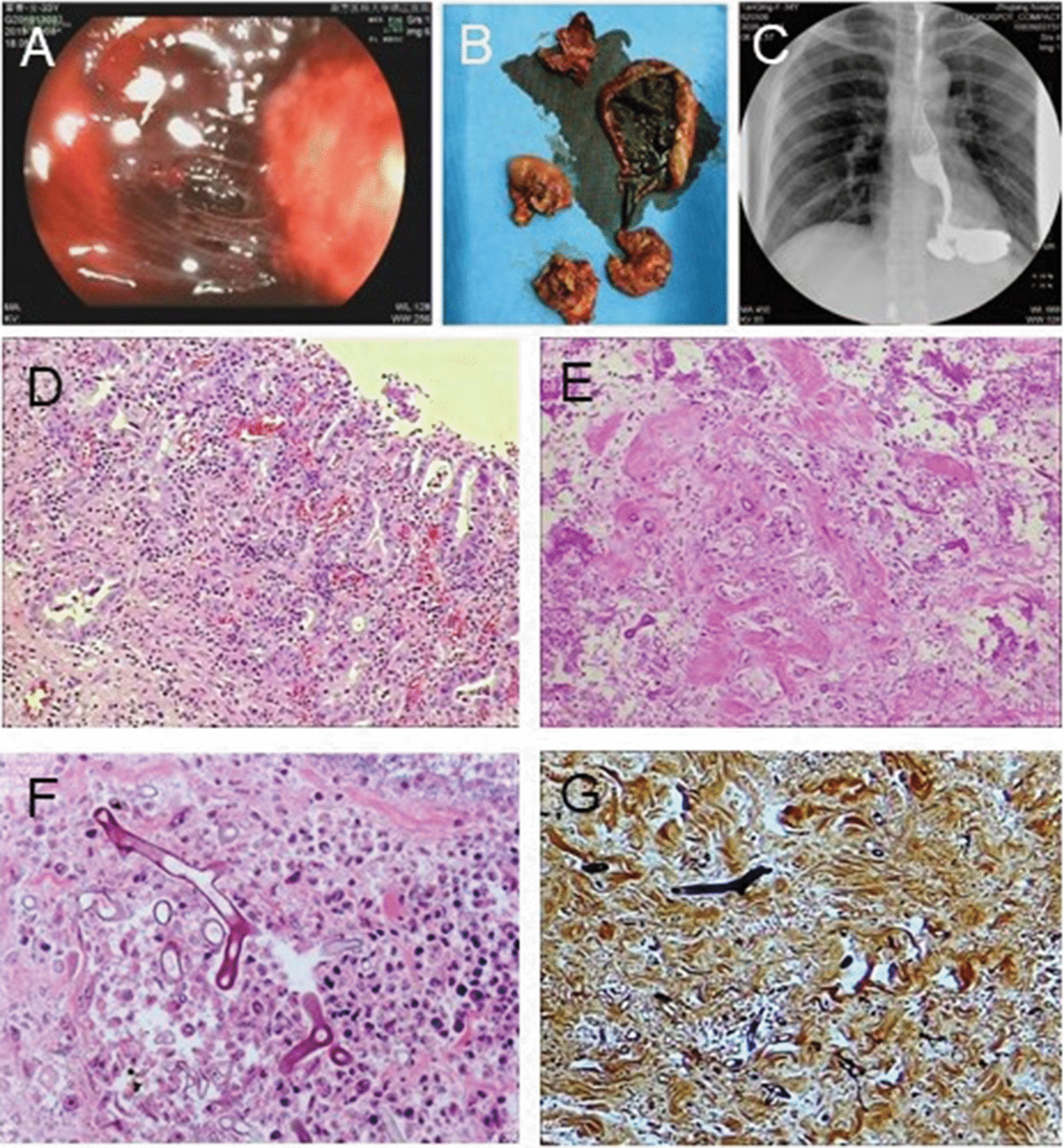
Case presentation: The first case was that of a 16-year-old immunocompetent boy who was admitted with gastrointestinal bleeding and perforation due to a gastric ulcer. Strategies used to arrest bleeding during emergency gastroscopy were unsuccessful. An adhesive mass was then discovered through laparoscopy. The patient underwent type II gastric resection. Pathological examination of the mass revealed bacterial infection and GIM. The second case was of a 33-year-old immunocompetent woman with a recent history of a lower leg sprain. The patient subsequently became critically ill and required ventilatory support. After hemodynamic stabilization and extubation, she presented with hematemesis due to exfoliation and necrosis of the stomach wall. The patient underwent total gastrectomy plus jejunostomy. The pathology results revealed severe bacterial infection and fungal infection that was confirmed as GIM. The patient fully recovered after receiving anti-infective and antifungal treatments.
Conclusions: Neither patient was immunosuppressed, and both patients presented with gastrointestinal bleeding. GIM was confirmed via pathological examination. GIM is not limited to immunocompromised patients, and its diagnosis mainly relies on pathological examination. Early diagnosis, timely surgical treatment, and early administration of systemic drug treatment are fundamental to improving its prognosis.
Keywords: Gastrointestinal bleeding; Gastrointestinal mucormycosis; Gastrointestinal perforation; Mucor; Mucormycosis.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
