

An in situ tissue engineering scaffold with growth factors combining angiogenesis and osteoimmunomodulatory functions for advanced periodontal bone regeneration
- PMID: 34404409
- PMCID: PMC8371786
- DOI: 10.1186/s12951-021-00992-4
An in situ tissue engineering scaffold with growth factors combining angiogenesis and osteoimmunomodulatory functions for advanced periodontal bone regeneration
Abstract
Background: The regeneration of periodontal bone defect remains a vital clinical challenge. To date, numerous biomaterials have been applied in this field. However, the immune response and vascularity in defect areas may be key factors that are overlooked when assessing the bone regeneration outcomes of biomaterials. Among various regenerative therapies, the up-to-date strategy of in situ tissue engineering stands out, which combined scaffold with specific growth factors that could mimic endogenous regenerative processes.
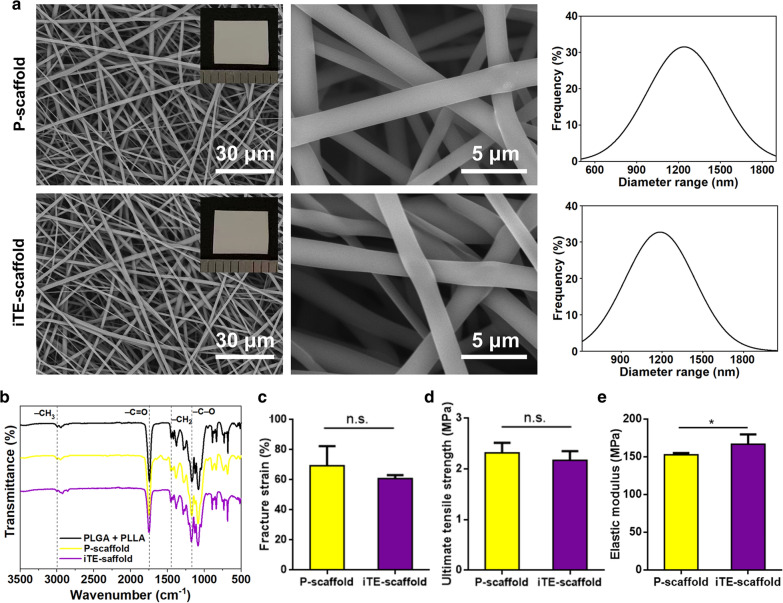
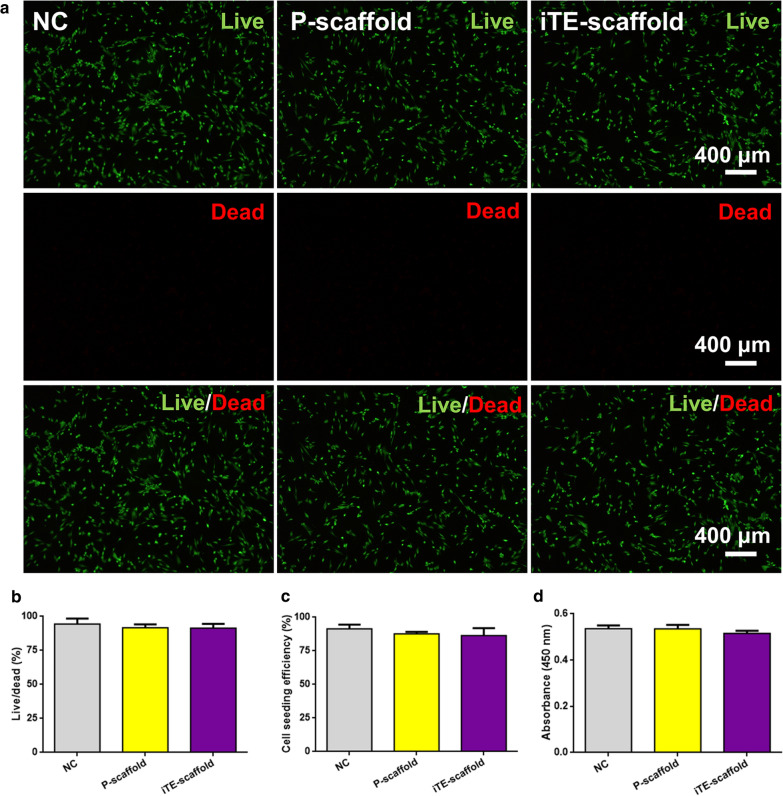
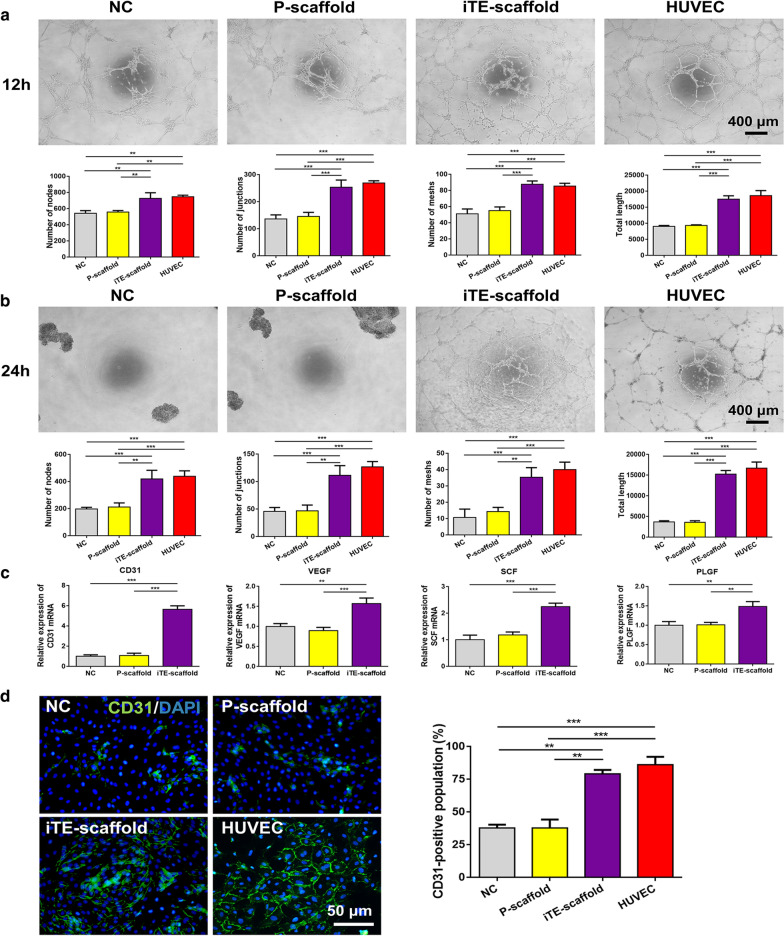
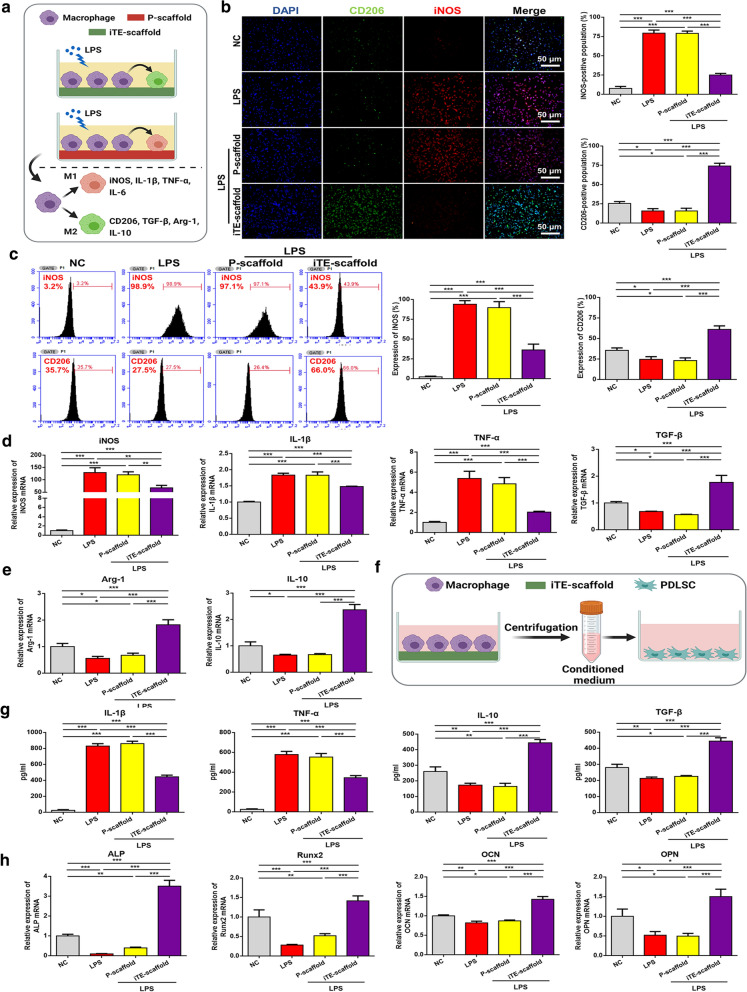
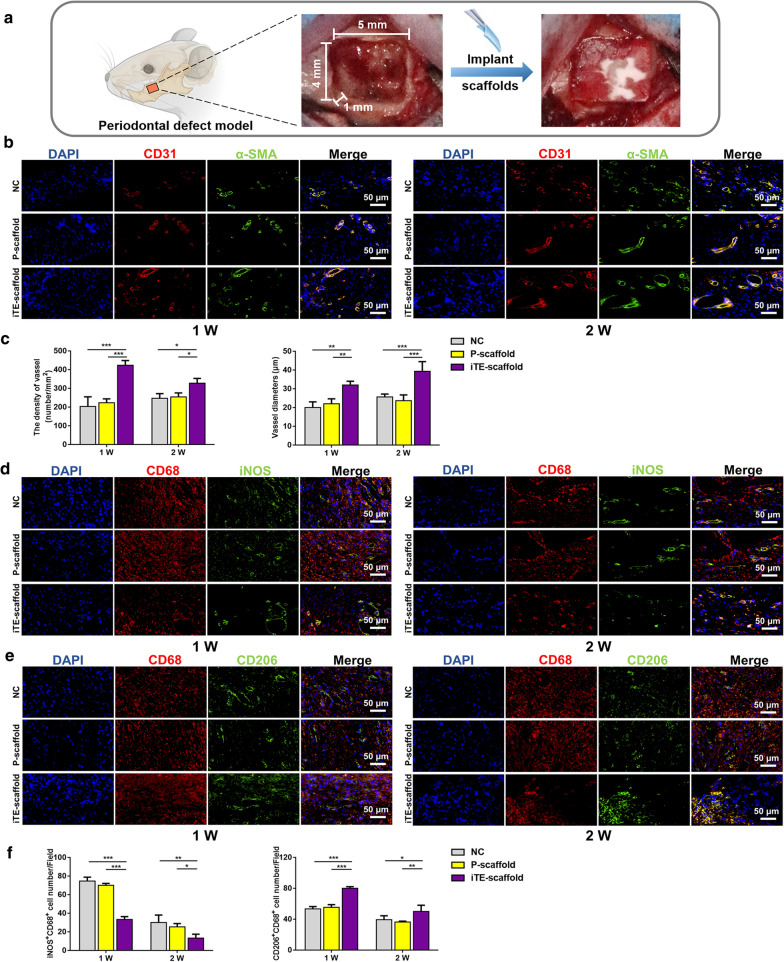
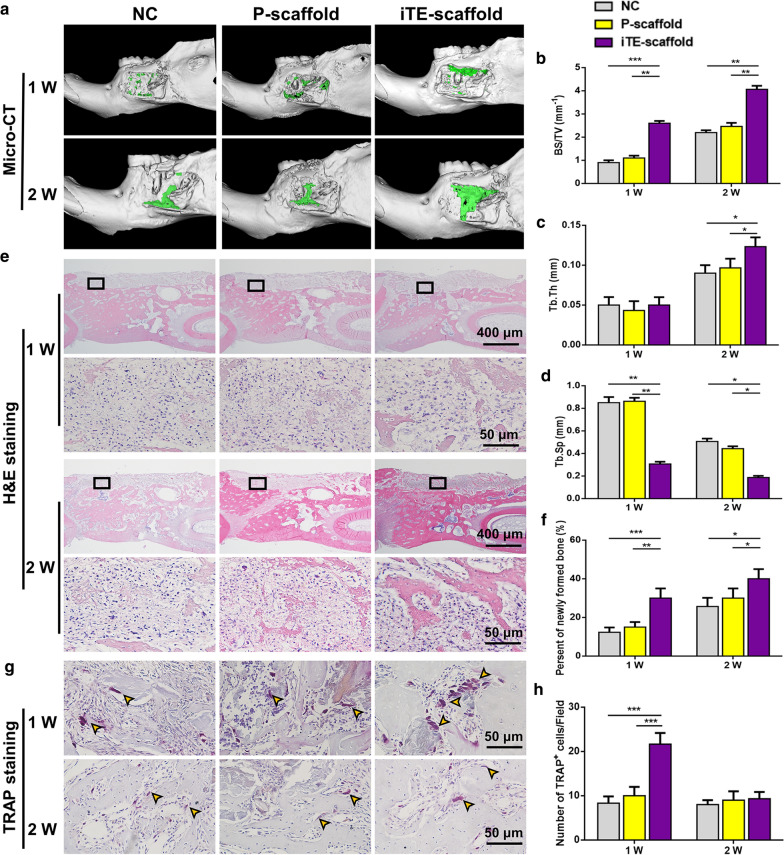
Results: Herein, we fabricated a core/shell fibrous scaffold releasing basic fibroblast growth factor (bFGF) and bone morphogenetic protein-2 (BMP-2) in a sequential manner and investigated its immunomodulatory and angiogenic properties during periodontal bone defect restoration. The in situ tissue engineering scaffold (iTE-scaffold) effectively promoted the angiogenesis of periodontal ligament stem cells (PDLSCs) and induced macrophage polarization into pro-healing M2 phenotype to modulate inflammation. The immunomodulatory effect of macrophages could further promote osteogenic differentiation of PDLSCs in vitro. After being implanted into the periodontal bone defect model, the iTE-scaffold presented an anti-inflammatory response, provided adequate blood supply, and eventually facilitated satisfactory periodontal bone regeneration.
Conclusions: Our results suggested that the iTE-scaffold exerted admirable effects on periodontal bone repair by modulating osteoimmune environment and angiogenic activity. This multifunctional scaffold holds considerable promise for periodontal regenerative medicine and offers guidance on designing functional biomaterials.
Keywords: Angiogenesis; Biomimetic repair; In situ tissue engineering; Osteoimmunomodulation; Periodontal bone regeneration.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing financial interest.
Figures
References
MeSH terms
Substances
Grants and funding
- 81873716/national natural science foundation of china
- ts20190975/tai'shan scholar engineering construction fund of shandong province of china
- tsqn201909180/tai'shan scholar engineering construction fund of shandong province of china
- ZR2020QH159/natural science foundation of shandong province
- 2017YFA0104604/national key research and development program of china
LinkOut - more resources
Full Text Sources
