

Estimate of the contemporary live-birth prevalence of recurrent 22q11.2 deletions: a cross-sectional analysis from population-based newborn screening
- PMID: 34404688
- PMCID: PMC8373039
- DOI: 10.9778/cmajo.20200294
Estimate of the contemporary live-birth prevalence of recurrent 22q11.2 deletions: a cross-sectional analysis from population-based newborn screening
Abstract
Background: Although pathogenic 22q11.2 deletions are an important cause of developmental delays and lifelong disease burden, their variable and complex clinical expression contributes to under-recognition, delayed molecular diagnosis and uncertainty about prevalence. We sought to estimate the contemporary live-birth prevalence of typical 22q11.2 deletions using a population-based newborn screening sample and to examine data available for associated clinical features.
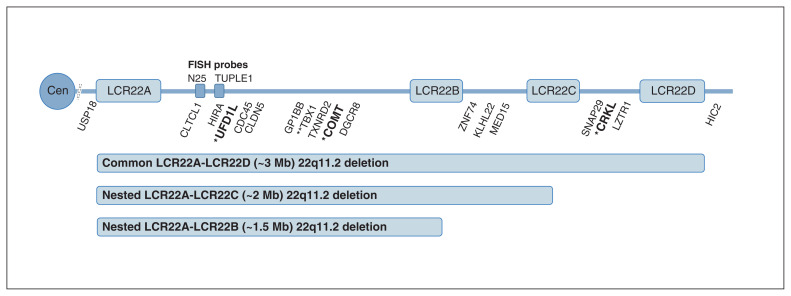
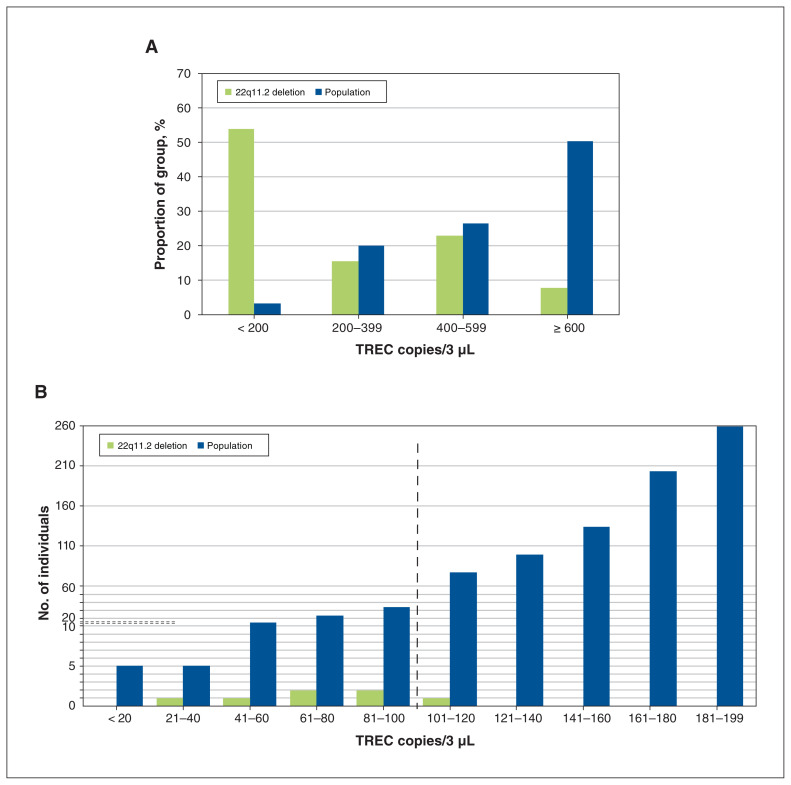
Methods: Using DNA available from an unbiased sample of about 12% of all dried blood spots collected for newborn screening in Ontario between January 2017 and September 2018, we prospectively screened for 22q11.2 deletions using multiplex quantitative polymerase chain reaction assays and conducted independent confirmatory studies. We used cross-sectional analyses to compare available clinical and T-cell receptor excision circle (TREC, used in newborn screening for severe combined immunodeficiency) data between samples with and without 22q11.2 deletions.
Results: The estimated minimum prevalence of 22q11.2 deletions was 1 in 2148 (4.7 per 10 000) live births (95% confidence interval [CI] 2.5 to 7.8 per 10 000), based on a total of 30 074 samples screened, with 14 having confirmed 22q11.2 deletions. Of term singletons, samples with 22q11.2 deletions had significantly younger median maternal age (25.5 v. 32.0 yr, difference -6.5 yr, 95% CI -7 to -2 yr), a greater proportion with small birth weight for gestational age (odds ratio 7.00, 95% CI 2.36 to 23.18) and lower median TREC levels (108.9 v. 602.5 copies/3 μL, p < 0.001).
Interpretation: These results indicate that the 22q11.2 deletion syndrome is one of the most common of rare genetic conditions and may be associated with relatively younger maternal ages and with prenatal growth abnormalities. The findings support the public health importance of early - prenatal and neonatal - diagnosis that would enable prompt screening for and management of well-known actionable features associated with 22q11.2 deletions.
© 2021 CMA Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Botto LD, May K, Fernhoff PM, et al. A population-based study of the 22q11.2 deletion: phenotype, incidence, and contribution to major birth defects in the population. Pediatrics. 2003;112:101–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical