

Respiratory epithelial cell responses to SARS-CoV-2 in COVID-19
- PMID: 34404754
- PMCID: PMC9273148
- DOI: 10.1136/thoraxjnl-2021-217561
Respiratory epithelial cell responses to SARS-CoV-2 in COVID-19
Abstract
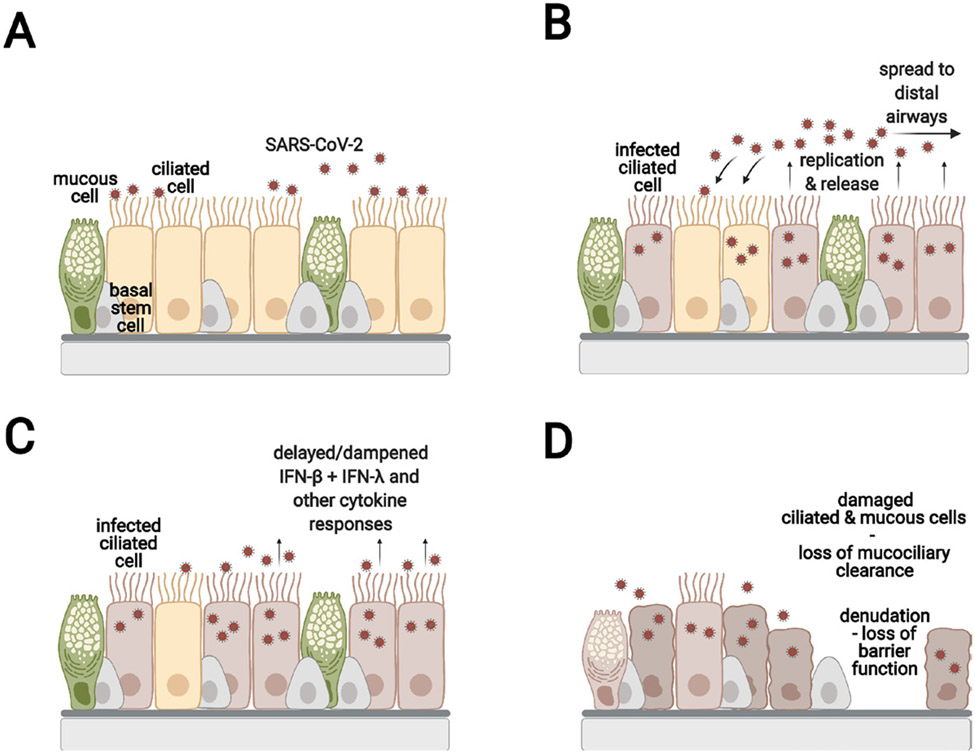
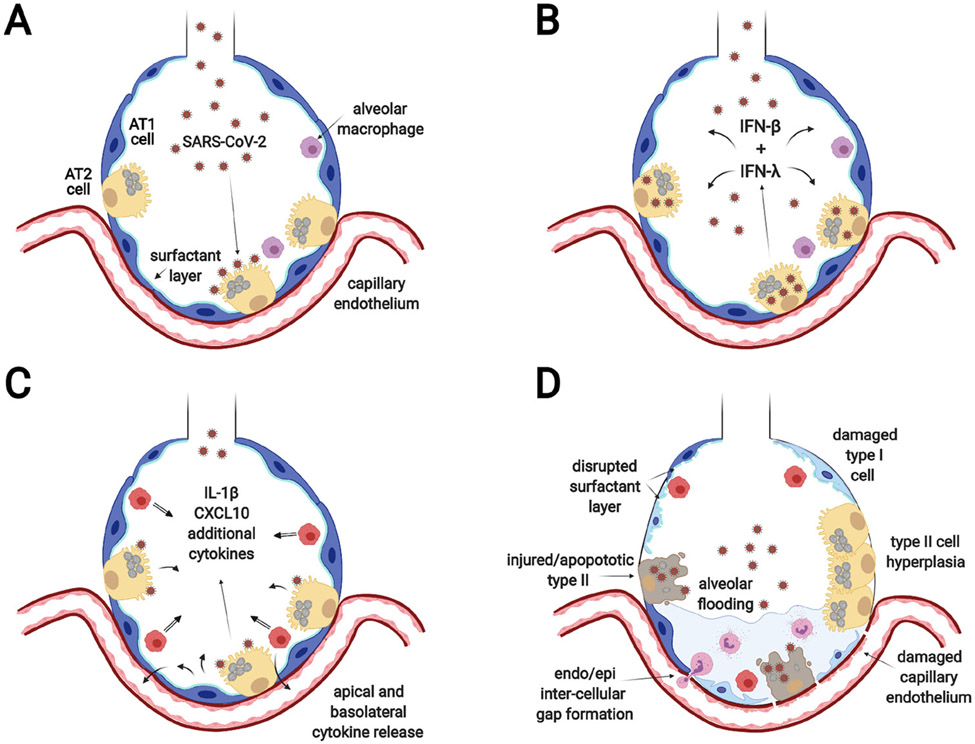
COVID-19 has different clinical stages, and effective therapy depends on the location and extent of the infection. The purpose of this review is to provide a background for understanding the progression of the disease throughout the pulmonary epithelium and discuss therapeutic options. The prime sites for infection that will be contrasted in this review are the conducting airways and the gas exchange portions of the lung. These two sites are characterised by distinct cellular composition and innate immune responses, which suggests the use of distinct therapeutic agents. In the nose, ciliated cells are the primary target cells for SARS-CoV-2 viral infection, replication and release. Infected cells shed their cilia, which disables mucociliary clearance. Evidence further points to a suppressed or incompletely activated innate immune response to SARS-CoV-2 infection in the upper airways. Asymptomatic individuals can still have a productive viral infection and infect others. In the gas exchange portion of the lung, the alveolar type II epithelial cell is the main target cell type. Cell death and marked innate immune response during infection likely contribute to alveolar damage and resultant acute respiratory distress syndrome. Alveolar infection can precipitate a hyperinflammatory state, which is the target of many therapies in severe COVID-19. Disease resolution in the lung is variable and may include scaring and long-term sequalae because the alveolar type II cells are also progenitor cells for the alveolar epithelium.
Keywords: ARDS; COVID-19; airway epithelium.
© Author(s) (or their employer(s)) 2022. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Wiersinga WJ, Rhodes A, Cheng AC, et al. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): a review. JAMA 2020;324:782–93. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous