

Efficacy of lenvatinib for unresectable hepatocellular carcinoma based on background liver disease etiology: multi-center retrospective study
- PMID: 34404856
- PMCID: PMC8370989
- DOI: 10.1038/s41598-021-96089-x
Efficacy of lenvatinib for unresectable hepatocellular carcinoma based on background liver disease etiology: multi-center retrospective study
Abstract
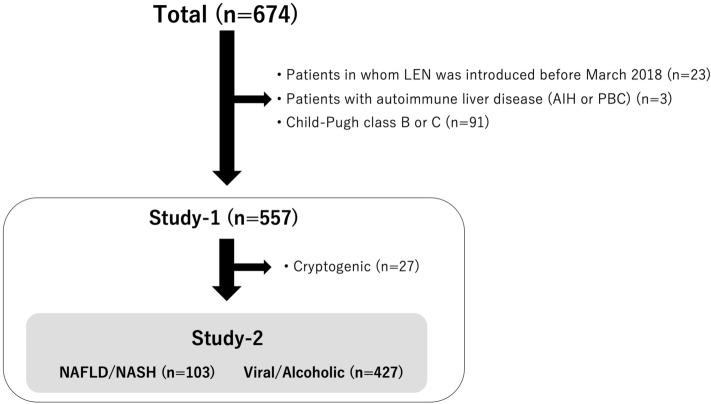
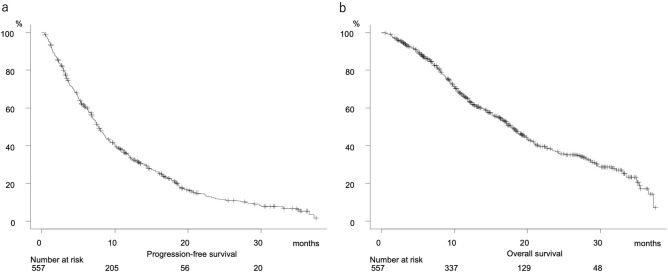
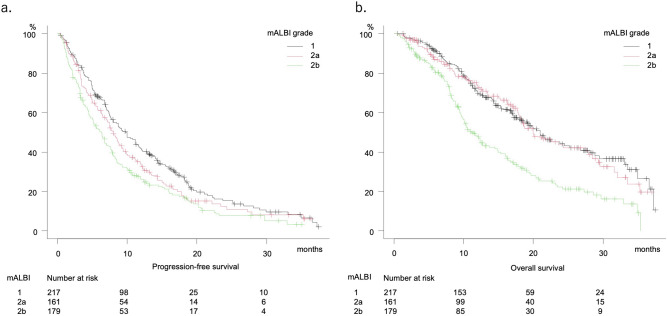
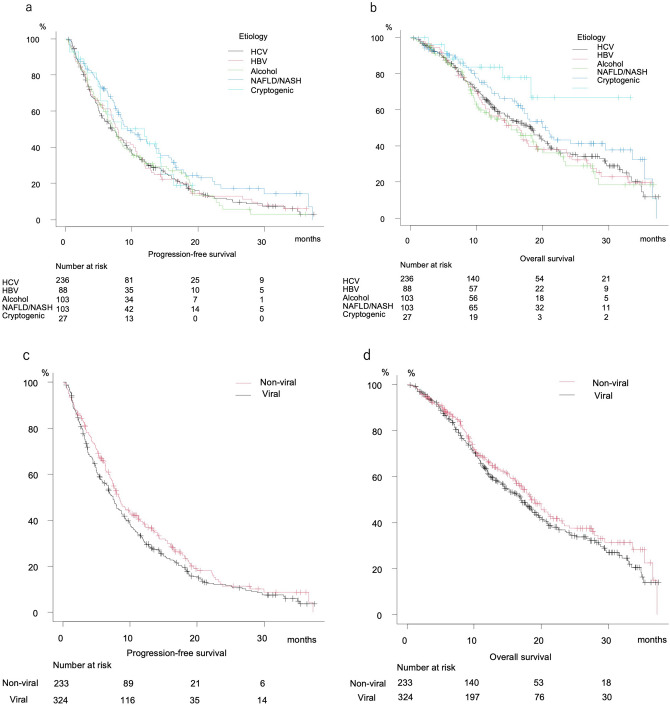
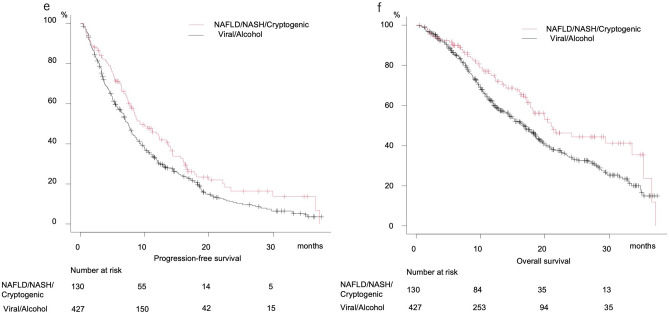
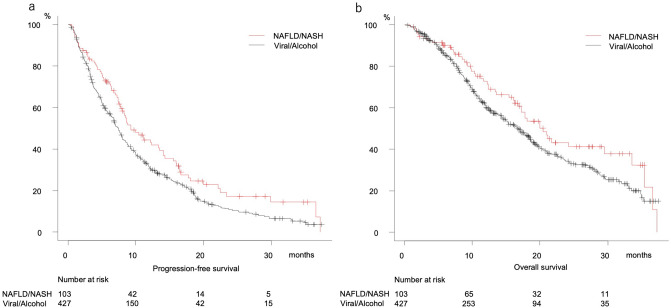
It was recently reported that hepatocellular carcinoma (HCC) patients with non-alcoholic steatohepatitis (NASH) are not responsive to immune-checkpoint inhibitor (ICI) treatment. The present study aimed to evaluate the therapeutic efficacy of lenvatinib in patients with non-alcoholic fatty liver disease (NAFLD)/NASH-related unresectable-HCC (u-HCC). Five hundred thirty u-HCC patients with Child-Pugh A were enrolled, and divided into the NAFLD/NASH (n = 103) and Viral/Alcohol (n = 427) groups. Clinical features were compared in a retrospective manner. Progression-free survival (PFS) was better in the NAFLD/NASH than the Viral/Alcohol group (median 9.3 vs. 7.5 months, P = 0.012), while there was no significant difference in overall survival (OS) (20.5 vs. 16.9 months, P = 0.057). In Cox-hazard analysis of prognostic factors for PFS, elevated ALT (≥ 30 U/L) (HR 1.247, P = 0.029), modified ALBI grade 2b (HR 1.236, P = 0.047), elevated AFP (≥ 400 ng/mL) (HR 1.294, P = 0.014), and NAFLD/NASH etiology (HR 0.763, P = 0.036) were significant prognostic factors. NAFLD/NASH etiology was not a significant prognostic factor in Cox-hazard analysis for OS (HR0.758, P = 0.092), whereas AFP (≥ 400 ng/mL) (HR 1.402, P = 0.009), BCLC C stage (HR 1.297, P = 0.035), later line use (HR 0.737, P = 0.014), and modified ALBI grade 2b (HR 1.875, P < 0.001) were significant. Lenvatinib can improve the prognosis of patients affected by u-HCC irrespective of HCC etiology or its line of treatment.
© 2021. The Author(s).
Conflict of interest statement
Atsushi Hiraoka, MD, PhD—Lecture fees: Bayer, Eisai, Eli Lilly, Otsuka. Takashi Kumada, MD, PhD—Lecture fees: Eisai. Masatoshi Kudo, MD, PhD—Advisory role: Eiasi, Ono, MSD, Bristol-Myers Squibb, Roche; Lecture fees: Eisai, Bayer, MSD, Bristol-Myers Squibb, Eli Lilly, EA Pharma; Research funding: Gilead Sciences, Taiho, Sumitomo Dainippon Pharma, Takeda, Otsuka, EA Pharma, Abbvie, Eisai. None of the other authors have potential conflicts of interest to declare.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
