

Clinical burden, risk factor impact and outcomes following myocardial infarction and stroke: A 25-year individual patient level linkage study
- PMID: 34405203
- PMCID: PMC8351196
- DOI: 10.1016/j.lanepe.2021.100141
Clinical burden, risk factor impact and outcomes following myocardial infarction and stroke: A 25-year individual patient level linkage study
Abstract
Background: Understanding trends in the incidence and outcomes of myocardial infarction and stroke, and how these are influenced by changes in cardiovascular risk factors can inform health policy and healthcare provision.
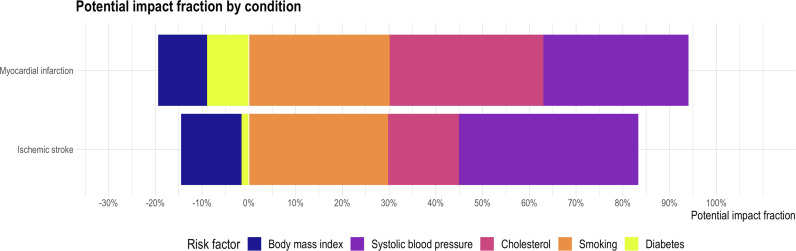
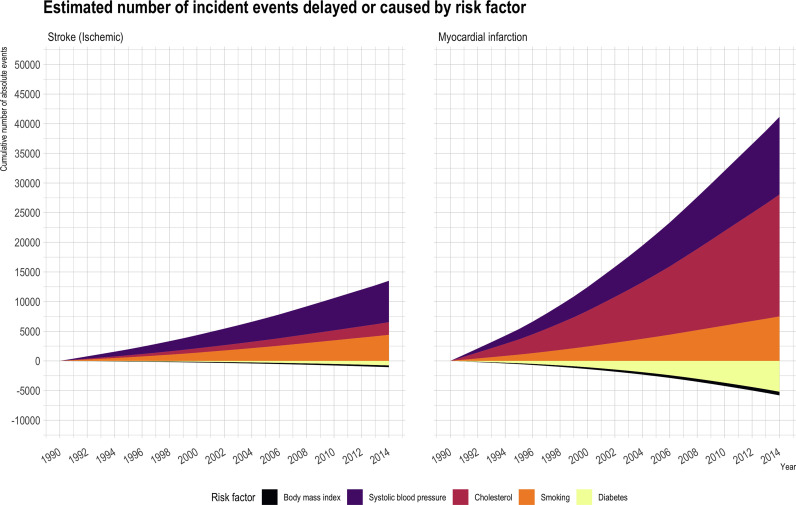
Methods: We identified all patients 30 years or older with myocardial infarction or stroke in Scotland. Risk factor levels were determined from national health surveys. Incidence, potential impact fractions and burden attributable to risk factor changes were calculated. Risk of subsequent fatal and non-fatal events (myocardial infarction, stroke, bleeding and heart failure hospitalization) were calculated with multi-state models.
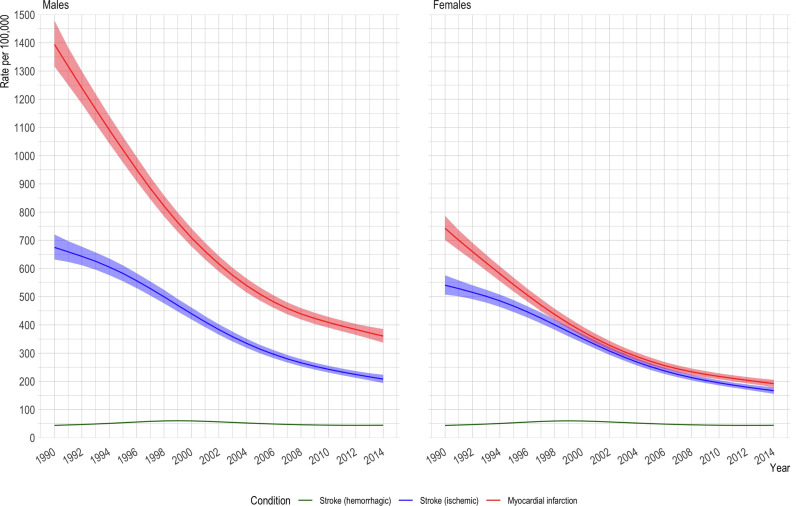
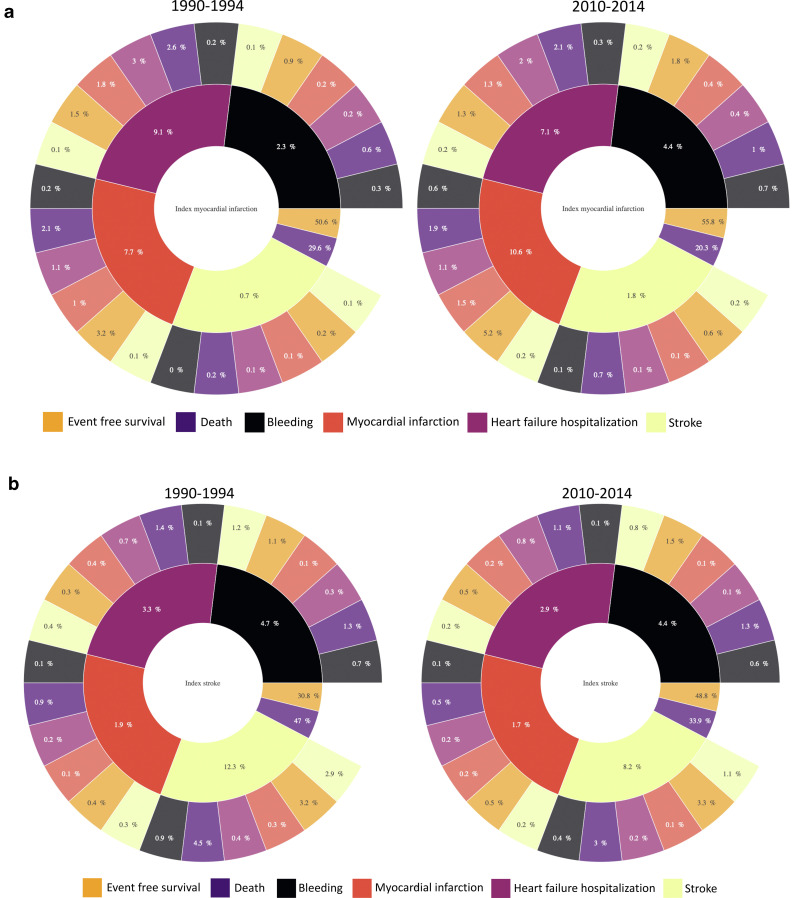
Findings: From 1990 to 2014, there were 372,873 (71±13 years) myocardial infarctions and 290,927 (74±13 years) ischemic or hemorrhagic strokes. Age-standardized incidence per 100,000 fell from 1,069 (95% confidence interval, 1,024-1,116) to 276 (263-290) for myocardial infarction and from 608 (581-636) to 188 (178-197) for ischemic stroke. Systolic blood pressure, smoking and cholesterol decreased, but body-mass index increased, and diabetes prevalence doubled. Changes in risk factors accounted for a 74% (57-91%) reduction in myocardial infarction and 68% (55-83%) reduction in ischemic stroke. Following myocardial infarction, the risk of death decreased (30% to 20%), but non-fatal events increased (20% to 24%) whereas the risk of both death (47% to 34%) and non-fatal events (22% to 17%) decreased following stroke.
Interpretation: Over the last 25 years, substantial reductions in myocardial infarction and ischemic stroke incidence are attributable to major shifts in risk factor levels. Deaths following the index event decreased for both myocardial infarction and stroke, but rates remained substantially higher for stroke.
Funding: British heart foundation.
© 2021 The Author(s).
Figures
References
-
- Rothwell PM, Coull AJ, Silver LE. Population-based study of event-rate, incidence, case fatality, and mortality for all acute vascular events in all arterial territories (Oxford Vascular Study) Lancet. 2005;366:1773–1783. - PubMed
-
- Falkeborn M, Persson I, Terent A, Bergstrom R, Lithell H, Naessen T. Long-term trends in incidence of and mortality from acute myocardial infarction and stroke in women: Analyses of total first events and of deaths in the Uppsala Health Care Region, Sweden. Epidemiology. 1996;7:67–74. - PubMed
-
- Hata J, Ninomiya T, Hirakawa Y. Secular trends in cardiovascular disease and its risk factors in Japanese: half-century data from the HisayamaStudy (1961-2009) Circulation. 2013;128:1198–1205. - PubMed
-
- Hunink MG, Goldman L, Tosteson AN. The recent decline in mortality from coronary heart disease, 1980-1990.The effect of secular trends in risk factors and treatment. JAMA. 1997;277:535–542. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
