

A Comprehensive Comparison of Early-Onset and Average-Onset Colorectal Cancers
- PMID: 34405229
- PMCID: PMC8634406
- DOI: 10.1093/jnci/djab124
A Comprehensive Comparison of Early-Onset and Average-Onset Colorectal Cancers
Abstract
Background: The causative factors for the recent increase in early-onset colorectal cancer (EO-CRC) incidence are unknown. We sought to determine if early-onset disease is clinically or genomically distinct from average-onset colorectal cancer (AO-CRC).
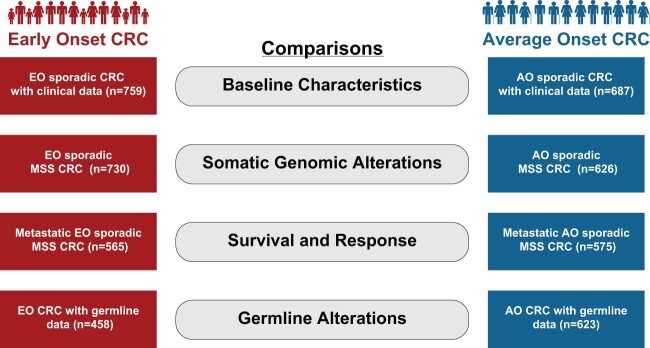
Methods: Clinical, histopathologic, and genomic characteristics of EO-CRC patients (2014-2019), divided into age 35 years and younger and 36-49 years at diagnosis, were compared with AO-CRC (50 years and older). Patients with mismatch repair deficient tumors, CRC-related hereditary syndromes, and inflammatory bowel disease were excluded from all but the germline analysis. All statistical tests were 2-sided.
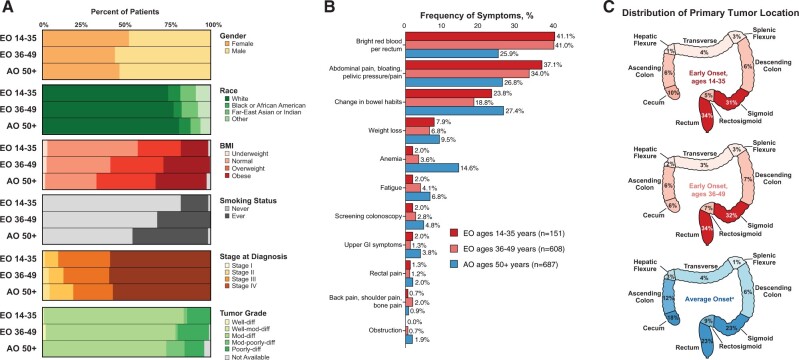
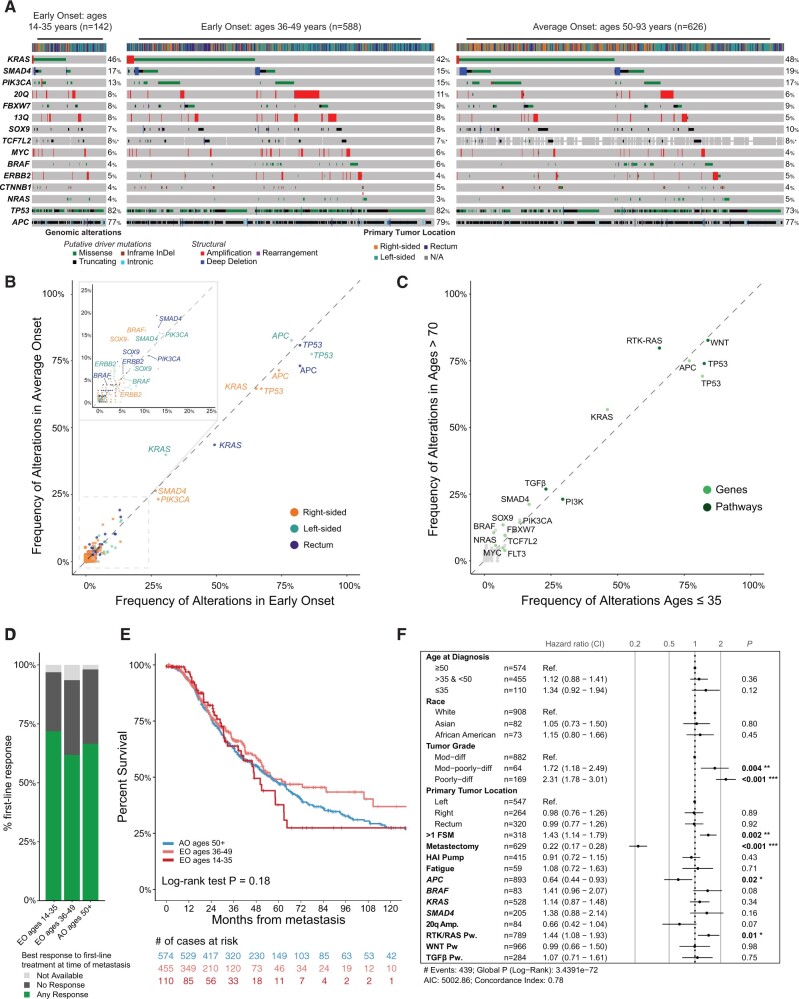
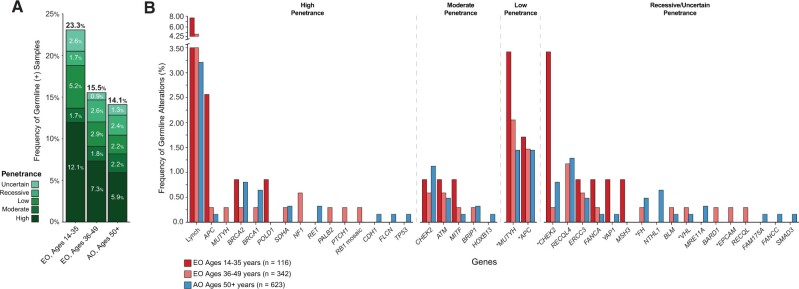
Results: In total, 759 patients with EO-CRC (35 years, n = 151; 36-49 years, n = 608) and AO-CRC (n = 687) were included. Left-sided tumors (35 years and younger = 80.8%; 36-49 years = 83.7%; AO = 63.9%; P < .001 for both comparisons), rectal bleeding (35 years and younger = 41.1%; 36-49 years = 41.0%; AO = 25.9%; P = .001 and P < .001, respectively), and abdominal pain (35 years and younger = 37.1%; 36-49 years = 34.0%; AO = 26.8%; P = .01 and P = .005, respectively) were more common in EO-CRC. Among microsatellite stable tumors, we found no differences in histopathologic tumor characteristics. Initially, differences in TP53 and Receptor Tyrosine Kinase signaling pathway (RTK-RAS)alterations were noted by age. However, on multivariate analysis including somatic gene analysis and tumor sidedness, no statistically significant differences at the gene or pathway level were demonstrated. Among advanced microsatellite stable CRCs, chemotherapy response and survival were equivalent by age cohorts. Pathogenic germline variants were identified in 23.3% of patients 35 years and younger vs 14.1% of AO-CRC (P = .01).
Conclusions: EO-CRCs are more commonly left-sided and present with rectal bleeding and abdominal pain but are otherwise clinically and genomically indistinguishable from AO-CRCs. Aggressive treatment regimens based solely on the age at CRC diagnosis are not warranted.
© The Author(s) 2021. Published by Oxford University Press. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Siegel RL, Miller KD, Goding Sauer A, et al. Colorectal cancer statistics, 2020. CA A Cancer J Clin. 2020;70(3):145–164. - PubMed
-
- Siegel RL, Jemal A, Ward EM.. Increase in incidence of colorectal cancer among young men and women in the United States. Cancer Epidemiol Biomarkers Prev. 2009;18(6):1695–1698. - PubMed
-
- Winawer SJ, Fletcher RH, Miller L, et al. Colorectal cancer screening: clinical guidelines and rationale. Gastroenterology. 1997;112(2):594–642. - PubMed
-
- Smith RA, Cokkinides V, Eyre HJ; for the American Cancer Society. American Cancer Society guidelines for the early detection of cancer, 2003. CA Cancer J Clin. 2003;53(1):27–43. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
