

Ten-year all-cause death after percutaneous or surgical revascularization in diabetic patients with complex coronary artery disease
- PMID: 34405232
- PMCID: PMC8720143
- DOI: 10.1093/eurheartj/ehab441
Ten-year all-cause death after percutaneous or surgical revascularization in diabetic patients with complex coronary artery disease
Abstract
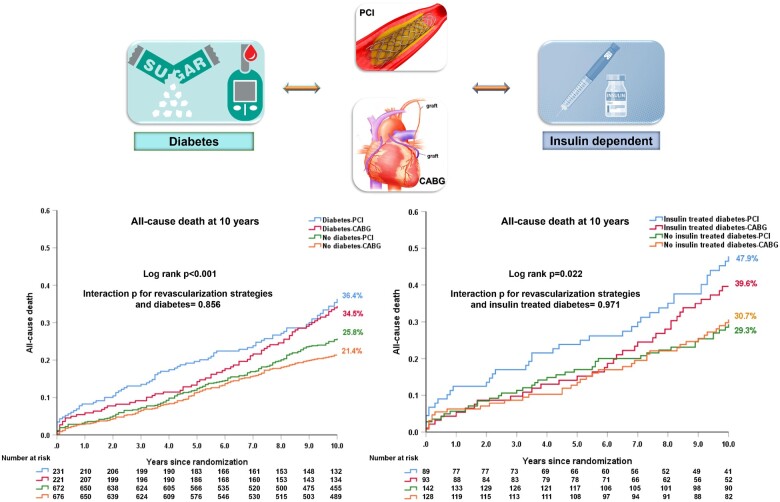
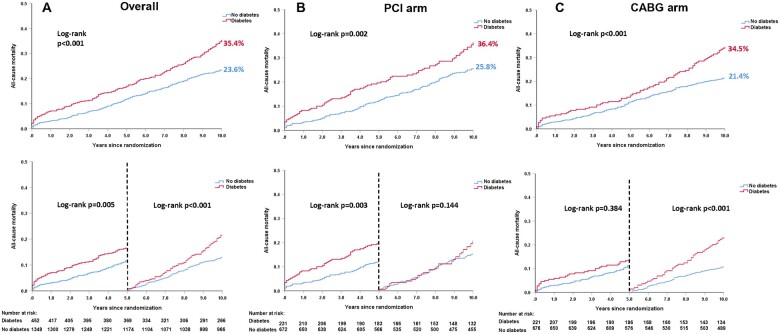
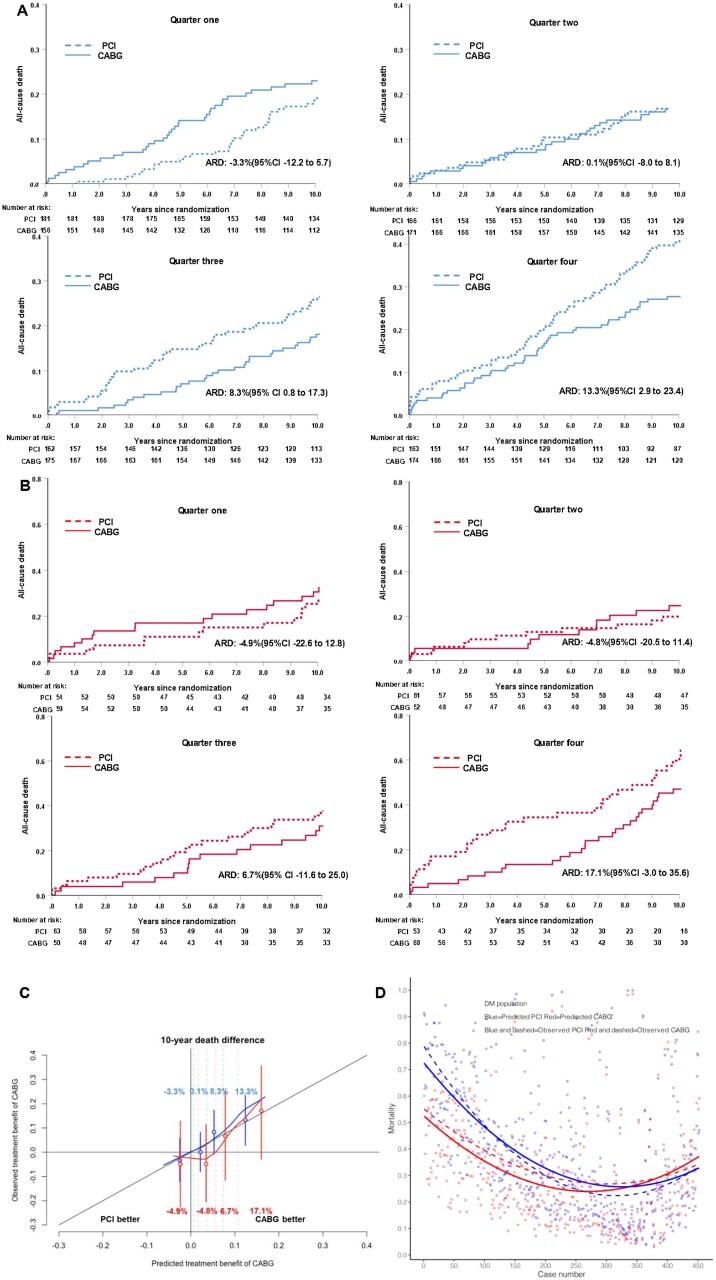
Aims: The aim of this article was to compare rates of all-cause death at 10 years following coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI) in patients with or without diabetes.
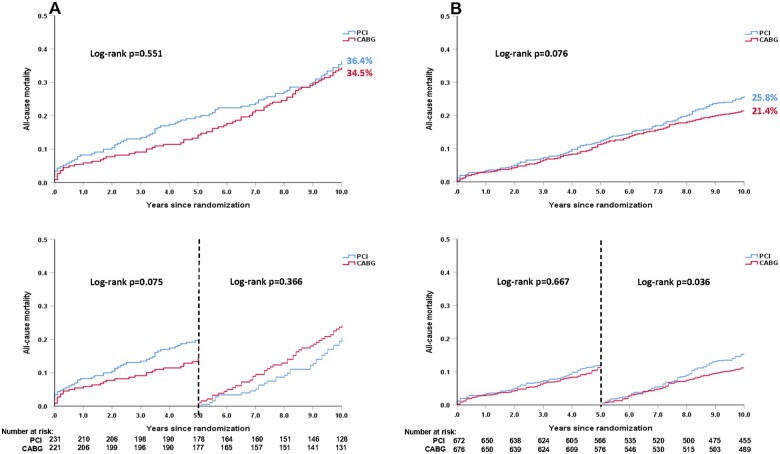
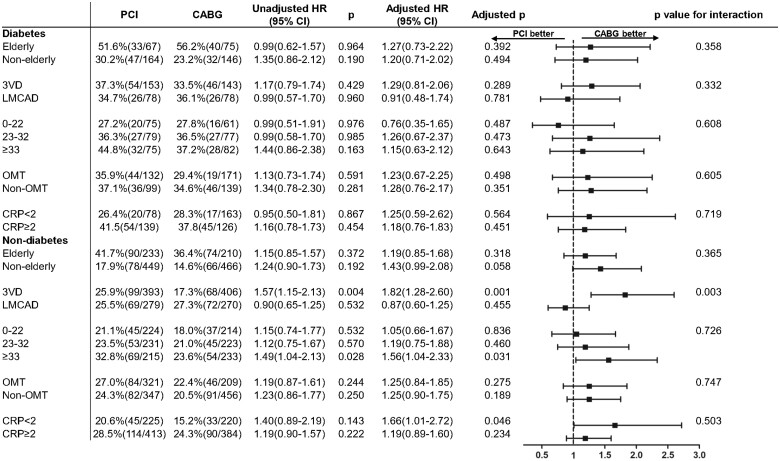
Methods and results: The SYNTAXES study evaluated up to 10-year survival of 1800 patients with three-vessel disease (3VD) and/or left main coronary artery disease (LMCAD) randomized to receive either PCI or CABG in the SYNTAX trial. Ten-year all-cause death according to diabetic status and revascularization strategy was examined. In diabetics (n = 452), the risk of mortality was numerically higher with PCI compared with CABG at 5 years [19.6% vs. 13.3%, hazard ratio (HR): 1.53, 95% confidence interval (CI): 0.96, 2.43, P = 0.075], with the opposite seen between 5 and 10 years (PCI vs. CABG: 20.8% vs. 24.4%, HR: 0.82, 95% CI: 0.52, 1.27, P = 0.366). Irrespective of diabetic status, there was no significant difference in all-cause death at 10 years between patients receiving PCI or CABG, the absolute treatment difference was 1.9% in diabetics (PCI vs. CABG: 36.4% vs. 34.5%, difference: 1.9%, 95% CI: -7.6%, 11.1%, P = 0.551). Among insulin-treated patients (n = 182), all-cause death at 10 years was numerically higher with PCI (47.9% vs. 39.6%, difference: 8.2%, 95% CI: -6.5%, 22.5%, P = 0.227).
Conclusions: The treatment effects of PCI vs. CABG on all-cause death at 10 years in patients with 3VD and/or LMCAD were similar irrespective of the presence of diabetes. There may, however, be a survival benefit with CABG in patients with insulin-treated diabetes. The association between revascularization strategy and very long-term ischaemic and safety outcomes for patients with diabetes needs further investigation in dedicated trials.
Trial registration: SYNTAX: ClinicalTrials.gov reference: NCT00114972 and SYNTAX Extended Survival: ClinicalTrials.gov reference: NCT03417050.
Keywords: All-cause death; Coronary artery bypass grafting; Diabetes; Percutaneous coronary intervention; SYNTAX.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Is there equivalence between PCI and CABG surgery in long-term survival of patients with diabetes? Importance of interpretation biases and biological plausibility.Eur Heart J. 2021 Dec 28;43(1):68-70. doi: 10.1093/eurheartj/ehab445. Eur Heart J. 2021. PMID: 34405227 No abstract available.
References
-
- Roffi M, Angiolillo DJ, Kappetein AP. Current concepts on coronary revascularization in diabetic patients. Eur Heart J 2011;32:2748–2757. - PubMed
-
- Kapur A, Hall RJ, Malik IS, Qureshi AC, Butts J, de Belder M, Baumbach A, Angelini G, de Belder A, Oldroyd KG, Flather M, Roughton M, Nihoyannopoulos P, Bagger JP, Morgan K, Beatt KJ. Randomized comparison of percutaneous coronary intervention with coronary artery bypass grafting in diabetic patients. 1-year results of the CARDia (Coronary Artery Revascularization in Diabetes) trial. J Am Coll Cardiol 2010;55:432–440. - PubMed
-
- Farkouh ME, Domanski M, Sleeper LA, Siami FS, Dangas G, Mack M, Yang M, Cohen DJ, Rosenberg Y, Solomon SD, Desai AS, Gersh BJ, Magnuson EA, Lansky A, Boineau R, Weinberger J, Ramanathan K, Sousa JE, Rankin J, Bhargava B, Buse J, Hueb W, Smith CR, Muratov V, Bansilal S, King S 3rd, Bertrand M, Fuster V; FREEDOM Trial Investigators. Strategies for multivessel revascularization in patients with diabetes. N Engl J Med 2012;367:2375–2384. - PubMed
-
- Kappetein AP, Head SJ, Morice MC, Banning AP, Serruys PW, Mohr FW, Dawkins KD, Mack MJ; on behalf of the SYNTAX Investigators. Treatment of complex coronary artery disease in patients with diabetes: 5-year results comparing outcomes of bypass surgery and percutaneous coronary intervention in the SYNTAX trial. Eur J Cardiothorac Surg 2013;43:1006–1013. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
