Association of Statin Treatment With Progression of Coronary Atherosclerotic Plaque Composition
- PMID: 34406326
- PMCID: PMC8374741
- DOI: 10.1001/jamacardio.2021.3055
Association of Statin Treatment With Progression of Coronary Atherosclerotic Plaque Composition
Abstract
Importance: The density of atherosclerotic plaque forms the basis for categorizing calcified and noncalcified morphology of plaques.
Objective: To assess whether alterations in plaque across a range of density measurements provide a more detailed understanding of atherosclerotic disease progression.
Design, setting, and participants: This cohort study enrolled 857 patients who underwent serial coronary computed tomography angiography 2 or more years apart and had quantitative measurements of coronary plaques throughout the entire coronary artery tree. The study was conducted from 2013 to 2016 at 13 sites in 7 countries.
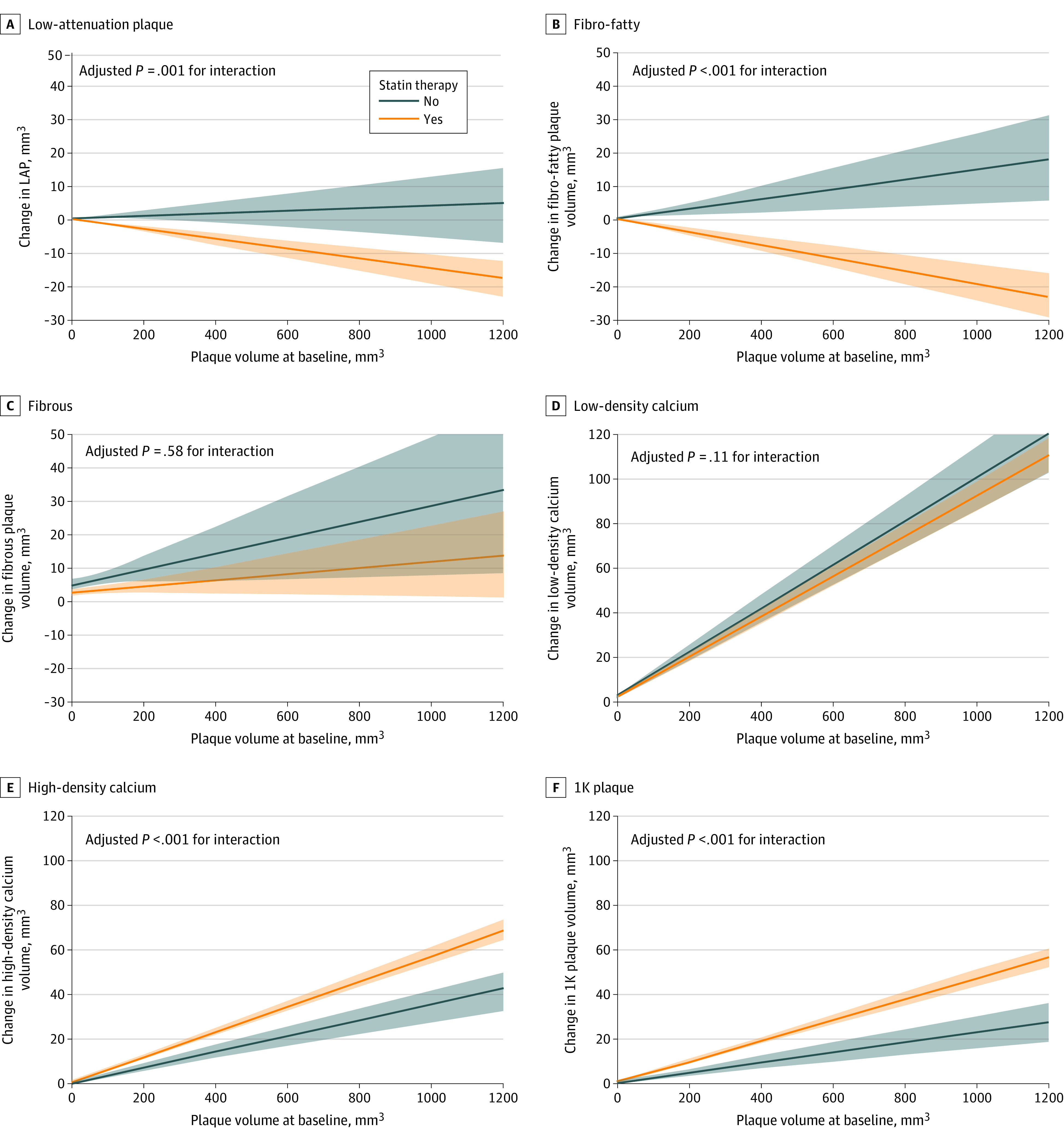
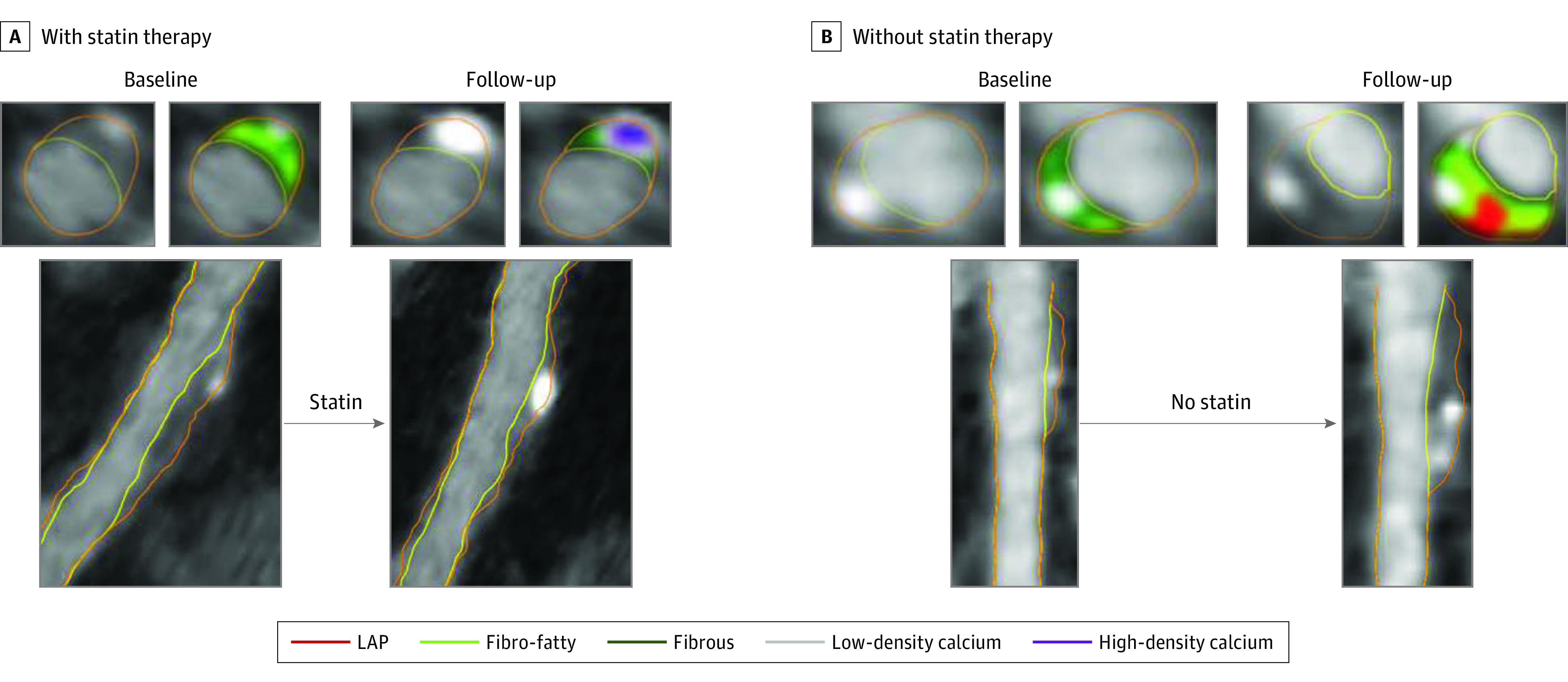
Main outcomes and measures: The main outcome was progression of plaque composition of individual coronary plaques. Six plaque composition types were defined on a voxel-level basis according to the plaque attenuation (expressed in Hounsfield units [HU]): low attenuation (-30 to 75 HU), fibro-fatty (76-130 HU), fibrous (131-350 HU), low-density calcium (351-700 HU), high-density calcium (701-1000 HU), and 1K (>1000 HU). The progression rates of these 6 compositional plaque types were evaluated according to the interaction between statin use and baseline plaque volume, adjusted for risk factors and time interval between scans. Plaque progression was also examined based on baseline calcium density. Analysis was performed among lesions matched at baseline and follow-up. Data analyses were conducted from August 2019 through March 2020.
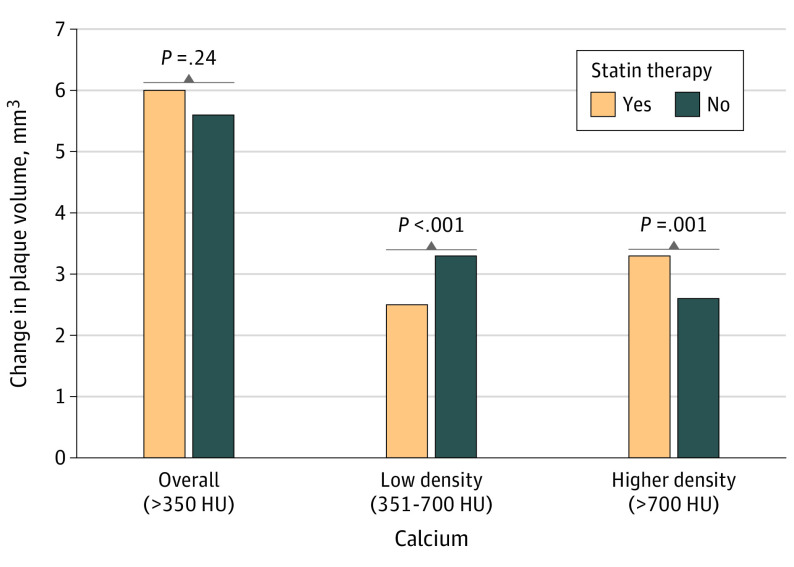
Results: In total, 2458 coronary lesions in 857 patients (mean [SD] age, 62.1 [8.7] years; 540 [63.0%] men; 548 [63.9%] received statin therapy) were included. Untreated coronary lesions increased in volume over time for all 6 compositional types. Statin therapy was associated with volume decreases in low-attenuation plaque (β, -0.02; 95% CI, -0.03 to -0.01; P = .001) and fibro-fatty plaque (β, -0.03; 95% CI, -0.04 to -0.02; P < .001) and greater progression of high-density calcium plaque (β, 0.02; 95% CI, 0.01-0.03; P < .001) and 1K plaque (β, 0.02; 95% CI, 0.01-0.03; P < .001). When analyses were restricted to lesions without low-attenuation plaque or fibro-fatty plaque at baseline, statin therapy was not associated with a change in overall calcified plaque volume (β, -0.03; 95% CI, -0.08 to 0.02; P = .24) but was associated with a transformation toward more dense calcium. Interaction analysis between baseline plaque volume and calcium density showed that more dense coronary calcium was associated with less plaque progression.
Conclusions and relevance: The results suggest an association of statin use with greater rates of transformation of coronary atherosclerosis toward high-density calcium. A pattern of slower overall plaque progression was observed with increasing density. All findings support the concept of reduced atherosclerotic risk with increased densification of calcium.
Conflict of interest statement
Figures