

Surface guided frameless positioning for lung stereotactic body radiation therapy
- PMID: 34406710
- PMCID: PMC8425933
- DOI: 10.1002/acm2.13370
Surface guided frameless positioning for lung stereotactic body radiation therapy
Abstract
Background and purpose: When treating lung tumors with stereotactic body radiation therapy (SBRT), patient immobilization is of outmost importance. In this study, the intra-fractional shifts of the patient (based on bony anatomy) and the tumor (based on the visible target volume) are quantified, and the associated impact on the delivered dose is estimated for a frameless immobilization approach in combination with surface guided radiation therapy (SGRT) monitoring.
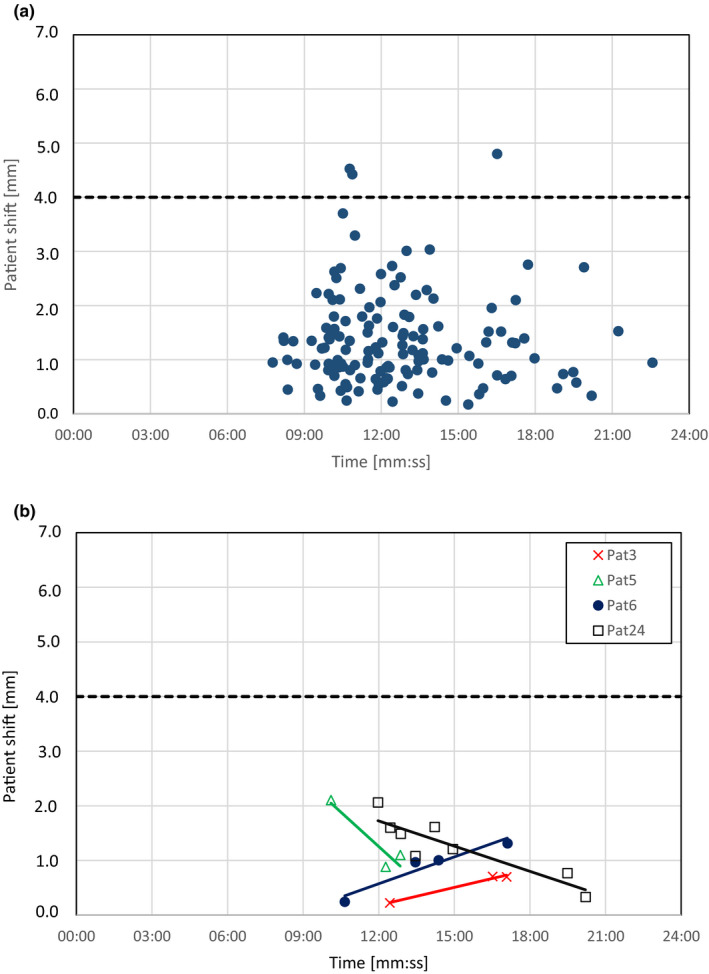
Methods: Cone beam computed tomographies (CBCT) were collected in free breathing prior and after each treatment for 25 patients with lung tumors, in total 137 fractions. The CBCT collected after each treatment was registered to the CBCT collected before each treatment with focus on bony anatomy to determine the shift of the patient, and with focus on the visible target volume to determine the shift of the tumor. Rigid registrations with 6 degrees of freedom were used. The patients were positioned in frameless immobilizations with their position and respiration continuously monitored by a commercial SGRT system. The patients were breathing freely within a preset gating window during treatment delivery. The beam was automatically interrupted if isocenter shifts >4 mm or breathing amplitudes outside the gating window were detected by the SGRT system. The time between the acquisition of the CBCTs was registered for each fraction to examine correlations between treatment time and patient shift. The impact of the observed shifts on the dose to organs at risk (OAR) and the gross tumor volume (GTV) was assessed.
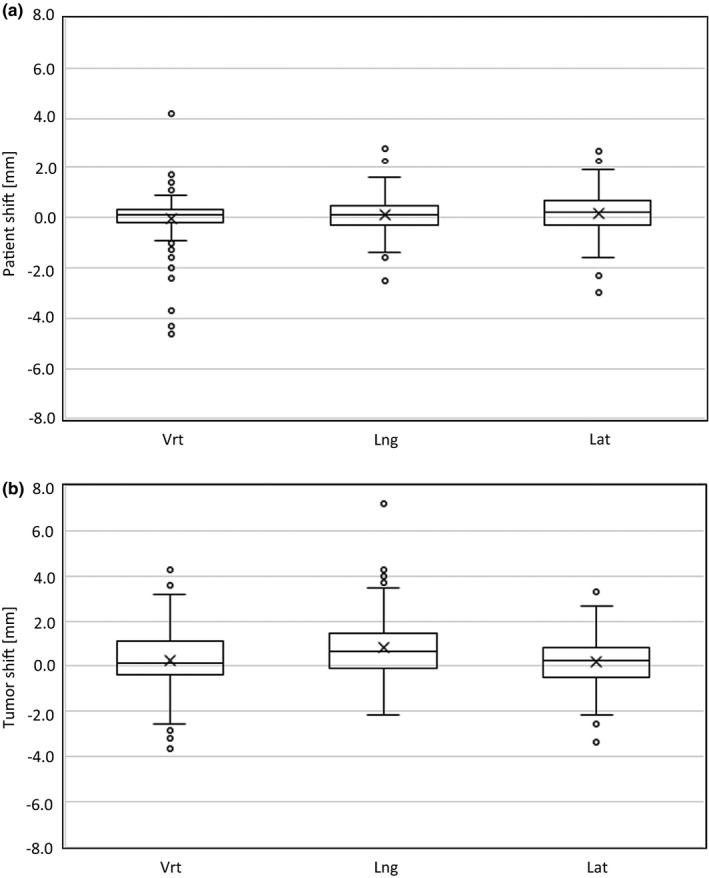
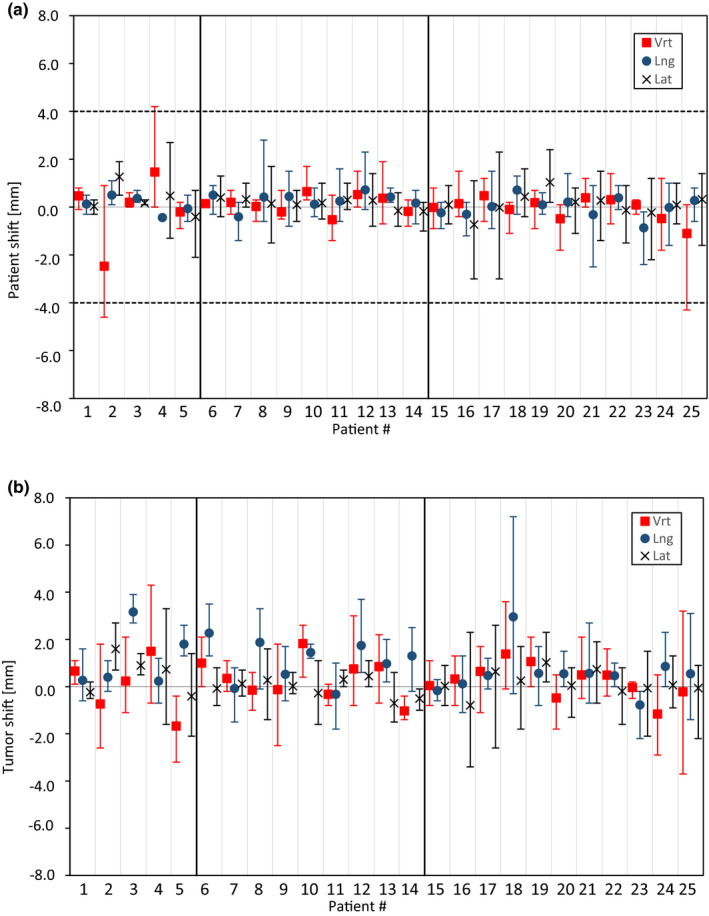
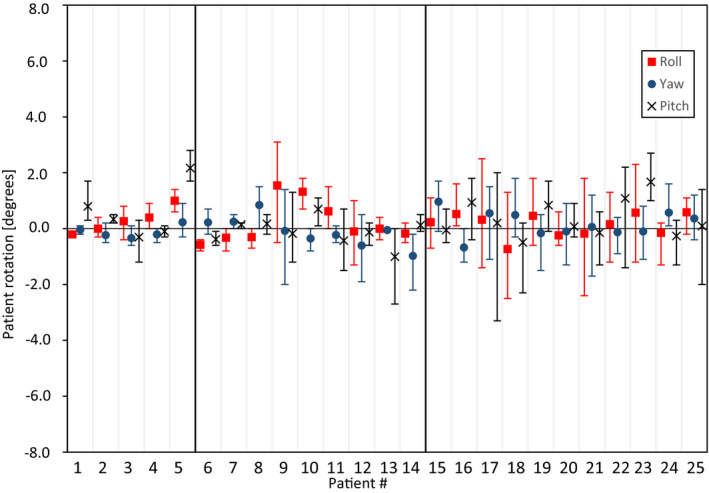
Results: The shift of the patient in the CBCTs was ≤2 mm for 132/137 fractions in the vertical (vrt) and lateral (lat) directions, and 134/137 fractions in the longitudinal (lng) direction and ≤4 mm in 134/137 (vrt) and 137/137 (lat, lng) of the fractions. The shift of the tumor was ≤2 mm in 116/137 (vrt), 123/137 (lat) and 115/137 (lng) fractions and ≤4 mm in 136/137 (vrt), 137/137 (lat), and 135/137 (lng) fractions. The maximal observed shift in the evaluated CBCT data was 4.6 mm for the patient and 7.2 mm for the tumor. Rotations were ≤3.3ᵒ for all fractions and the mean/standard deviation were 0.2/1.0ᵒ (roll), 0.1/0.8ᵒ (yaw), and 0.3/1.0ᵒ (pitch). The SGRT system interrupted the beam due to intra-fractional isocenter shifts >4 mm for 21% of the fractions, but the patients always returned within tolerance without the need of repositioning. The maximal observed isocenter shift by the SGRT system during the beam holds was 8 mm. For the respiration monitoring, the beam was interrupted at least one time for 54% of the fractions. The visual tumor was within the planned internal target volume (ITV) for 136/137 fractions in the evaluated CBCT data collected at the end of each fraction. For the fraction where the tumor was outside the ITV, the D98% for the GTV decreased with 0.4 Gy. For the OARs, the difference between planned and estimated dose from the CBCT data (D2% or Dmean ) was ≤2.6% of the prescribed PTV dose. No correlation was found between treatment time and the magnitude of the patient shift.
Conclusions: Using SGRT for motion management and respiration monitoring in combination with a frameless immobilization is a feasible approach for lung SBRT.
Keywords: SBRT; SGRT; immobilization; motion management.
© 2021 The Authors. Journal of Applied Clinical Medical Physics published by Wiley Periodicals LLC on behalf of American Association of Physicists in Medicine.
Conflict of interest statement
The authors have no relevant conflicts of interest to disclose.
Figures
References
-
- Zheng X, Schipper M, Kidwell K, et al. Survival outcome after stereotactic body radiation therapy and surgery for stage I non‐small cell lung cancer: a metaanalysis. Int J Radiat Oncol Biol Phys. 2014;90:603‐611. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
