

Mobile health assisted self-monitoring is acceptable for supporting weight loss in rural men: a pragmatic randomized controlled feasibility trial
- PMID: 34407782
- PMCID: PMC8375071
- DOI: 10.1186/s12889-021-11618-7
Mobile health assisted self-monitoring is acceptable for supporting weight loss in rural men: a pragmatic randomized controlled feasibility trial
Abstract
Background: Addressing overweight and obesity among men at-risk for obesity-related diseases and disability in rural communities is a public health issue. Commercial smartphone applications (apps) that promote self-monitoring for weight loss are widely available. Evidence is lacking regarding what support is required to enhance user engagement with and effectiveness of those technologies. Pragmatically comparing these apps effectiveness, including rural men's desired forms of support when using them, can lead to greater weight loss intervention impact and reach. This study assessed the feasibility and acceptability of a mobile technology application applied differently across two groups for weight loss.
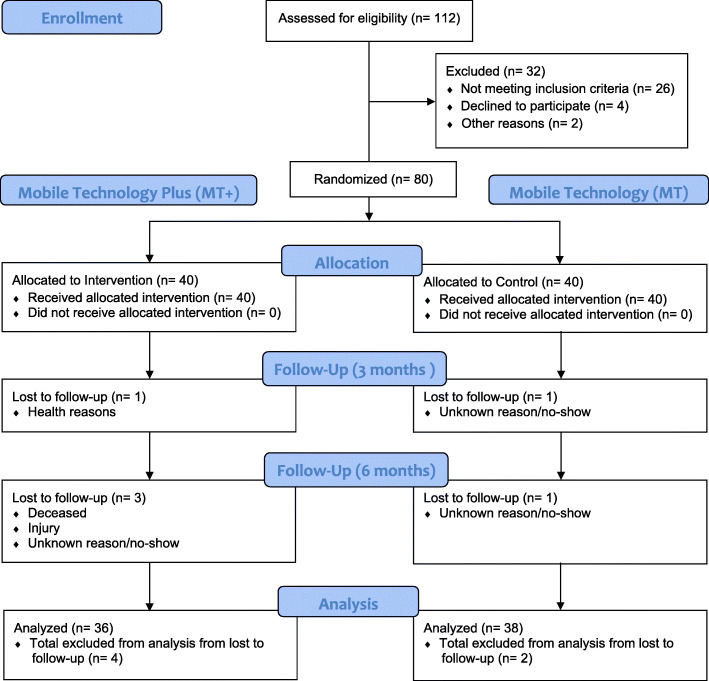
Methods: In a two-armed, pragmatic pilot feasibility study, 80 overweight and obese men aged 40-69 were randomized using a 1:1 ratio to either an enhanced Mobile Technology Plus (MT+) intervention or a basic Mobile Technology (MT) intervention. The MT+ group had an enhanced smartphone app for self-monitoring (text messaging, discussion group, Wi-Fi scale) whereas the MT group received a basic app that allowed self-monitoring logging only. Assessments were collected at baseline, 3 and 6 months. App logs were analyzed to track engagement and adherence to self-monitoring. Acceptability was assessed via focus groups. Analysis included descriptive statistics and qualitative content analysis.
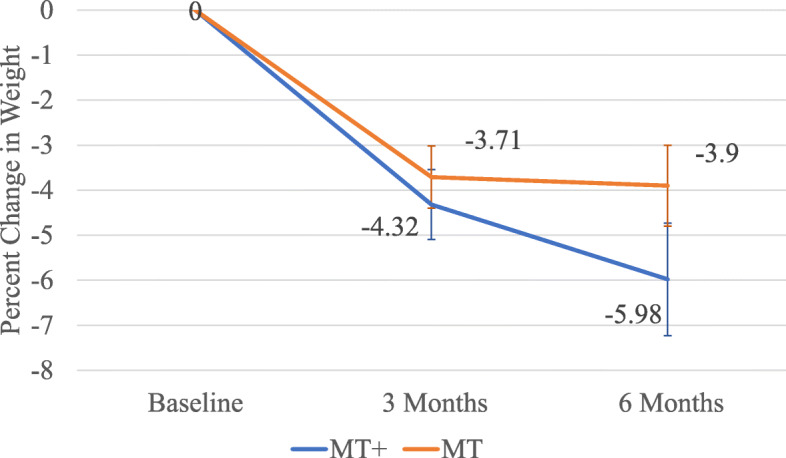
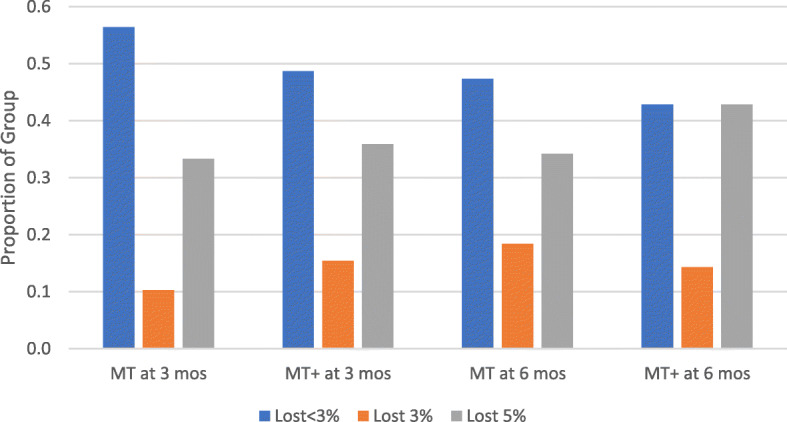
Results: Of 80 men recruited, forty were allocated to each arm. All were included in the primary analysis. Recruitment ended after 10 months with a 97.5 and 92.5% (3 month, 6 month) retention rate. Over 90% of men reported via survey and focus groups that Lose-It app and smart scale (MT+) was an acceptable way to self-monitor weight, dietary intake and physical activity. Adherence to daily app self-monitoring of at least 800 dietary calories or more (reported respectively as MT+, MT) was positive with 73.4, 51.6% tracking at least 5 days a week. Adherence to tracking activity via recorded steps four or more days weekly was positive, 87.8, 64.6%. Men also adhered to self-weighing at least once weekly, 64, 46.3%. At 6 months, an observed mean weight loss was 7.03 kg (95% CI: 3.67, 10.39) for MT+ group and 4.14 kg (95% CI: 2.22, 6.06) for MT group, with 42.9 and 34.2% meeting ≥5% weight loss, respectively. No adverse events were reported.
Conclusions: This National Institutes of Health-funded pilot study using mobile technologies to support behavior change for weight loss was found to be feasible and acceptable among midlife and older rural men. The interventions demonstrated successful reductions in weight, noting differing adherence to lifestyle behaviors of eating, monitoring and activity between groups, with men in the MT+ having more favorable results. These findings will be used to inform the design of a larger scale, clinical trial.
Trial registration: The trial was prospectively registered with ClinicalTrials NCT03329079 . 11/1/2017.
Keywords: Health disparities; Men; Mobile health technologies; Rural population; Self-monitoring; Weight loss.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Hales C, Carroll M, Fryar C, Ogden C. Prevalence of obesity among adults and youth: United States, 2015–2016. Hyattsville, MD: National Center for Health Statistics; 2017.
-
- Guo Z, Jiang Y, Huffman SK. Agricultural mechanization and BMI for rural workers: a field experiment in China. Economics Working Papers: Department of Economics, Iowa State University. 2018;(18010):1-23.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
