

Indirect comparison of TIMI, HEART and GRACE for predicting major cardiovascular events in patients admitted to the emergency department with acute chest pain: a systematic review and meta-analysis
- PMID: 34408048
- PMCID: PMC8375746
- DOI: 10.1136/bmjopen-2020-048356
Indirect comparison of TIMI, HEART and GRACE for predicting major cardiovascular events in patients admitted to the emergency department with acute chest pain: a systematic review and meta-analysis
Abstract
Background: The study aimed to compare the predictive values of the thrombolysis in myocardial infarction (TIMI); History, Electrocardiography, Age, Risk factors and Troponin (HEART) and Global Registry in Acute Coronary Events (GRACE) scoring systems for major adverse cardiovascular events (MACEs) in acute chest pain (ACP) patients admitted to the emergency department (ED).
Methods: We systematically searched PubMed, Embase and the Cochrane Library from their inception to June 2020; we compared the following parameters: sensitivity, specificity, positive and negative likelihood ratios (PLR and NLR), diagnostic OR (DOR) and area under the receiver operating characteristic curves (AUC).
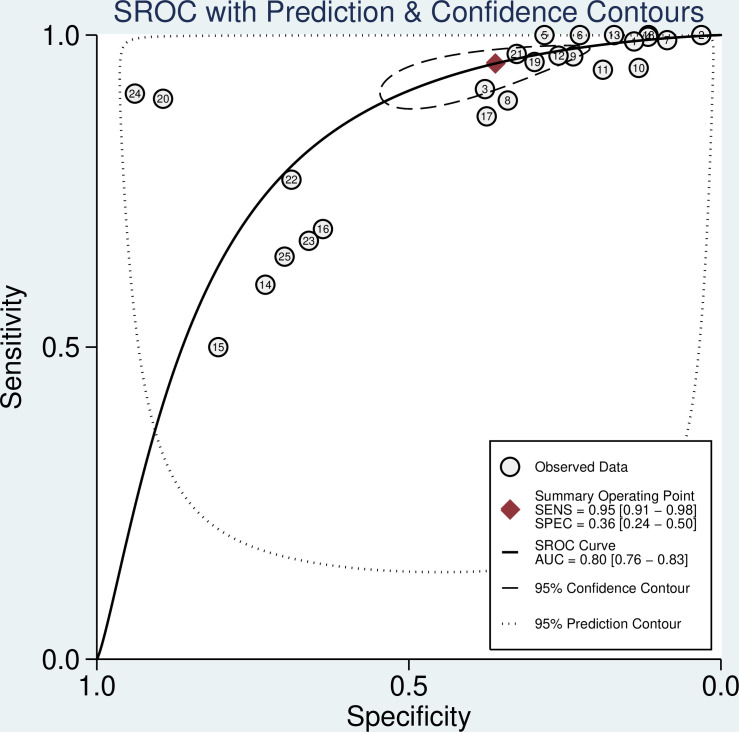
Results: The pooled sensitivity and specificity for TIMI, HEART and GRACE were 0.95 and 0.36, 0.96 and 0.50, and 0.78 and 0.56, respectively. The pooled PLR and NLR for TIMI, HEART and GRACE were 1.49 and 0.13, 1.94 and 0.08, and 1.77 and 0.40, respectively. The pooled DOR for TIMI, HEART and GRACE was 9.18, 17.92 and 4.00, respectively. The AUC for TIMI, HEART and GRACE was 0.80, 0.80 and 0.70, respectively. Finally, the results of indirect comparison suggested the superiority of values of TIMI and HEART to those of GRACE for predicting MACEs, while there were no significant differences between TIMI and HEART for predicting MACEs.
Conclusions: TIMI and HEART were superior to GRACE for predicting MACE risk in ACP patients admitted to the ED.
Keywords: accident & emergency medicine; adult cardiology; coronary heart disease.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures




References
-
- World Health Organization . Cardiovascular diseases. Available: https://www.who.int/en/news-room/fact-sheets/detail/cardiovascular-disea... [Accessed June 2019].
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical