

Association of Neighborhood-Level Material Deprivation With Health Care Costs and Outcome After Stroke
- PMID: 34408072
- PMCID: PMC8575135
- DOI: 10.1212/WNL.0000000000012676
Association of Neighborhood-Level Material Deprivation With Health Care Costs and Outcome After Stroke
Abstract
Background and objectives: To determine the association between material deprivation and direct health care costs and clinical outcomes following stroke in the context of a publicly funded universal health care system.
Methods: In this population-based cohort study of patients with ischemic and hemorrhagic stroke admitted to the hospital between 2008 and 2017 in Ontario, Canada, we used linked administrative data to identify the cohort, predictor variables, and outcomes. The exposure was a 5-level neighborhood material deprivation index. The primary outcome was direct health care costs incurred by the public payer in the first year. Secondary outcomes were death and admission to long-term care.
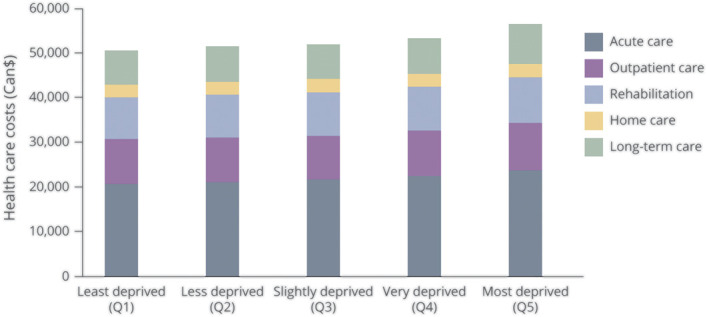
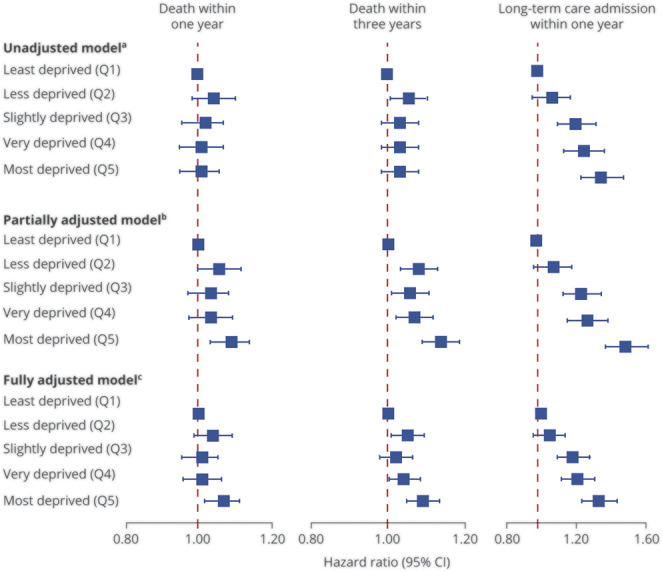
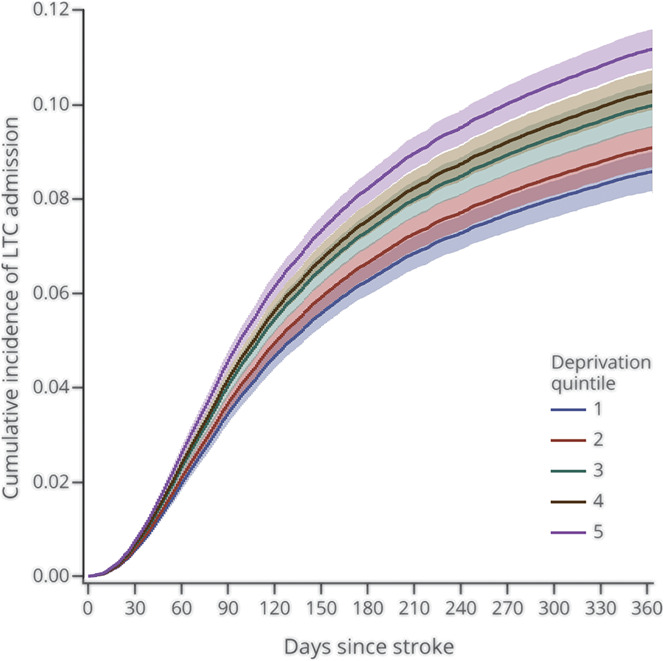
Results: Among 90,289 patients with stroke, the mean (SD) per-person costs increased with increasing material deprivation, from $50,602 ($55,582) in the least deprived quintile to $56,292 ($59,721) in the most deprived quintile (unadjusted relative cost ratio and 95% confidence interval 1.11 [1.08, 1.13] and adjusted relative cost ratio 1.07 [1.05, 1.10] for least compared to most deprived quintile). People in the most deprived quintile had higher mortality within 1 year compared to the least deprived quintile (adjusted hazard ratio [HR] 1.07 [1.03, 1.12]) as well as within 3 years (adjusted HR 1.09 [1.05, 1.13]). Admission to long-term care increased incrementally with material deprivation and those in the most deprived quintile had an adjusted HR of 1.33 (1.24, 1.43) compared to those in the least deprived quintile.
Discussion: Material deprivation is a risk factor for increased costs and poor outcomes after stroke. Interventions targeting health inequities due to social determinants of health are needed.
Classification of evidence: This study provides Class II evidence that the neighborhood-level material deprivation predicts direct health care costs.
© 2021 American Academy of Neurology.
Figures
Similar articles
-
Association of Neighborhood Deprivation With Thrombolysis and Thrombectomy for Acute Stroke in a Health System With Universal Access.Neurology. 2023 Nov 27;101(22):e2215-e2222. doi: 10.1212/WNL.0000000000207924. Neurology. 2023. PMID: 37914415 Free PMC article.
-
Association of Neighborhood-Level Material Deprivation With Atrial Fibrillation Care in a Single-Payer Health Care System: A Population-Based Cohort Study.Circulation. 2022 Jul 19;146(3):159-171. doi: 10.1161/CIRCULATIONAHA.122.058949. Epub 2022 Jun 9. Circulation. 2022. PMID: 35678171 Free PMC article.
-
Association of material deprivation with discharge location and length of stay after inpatient stroke rehabilitation in Ontario: a retrospective, population-based cohort study.CMAJ Open. 2022 Jan 25;10(1):E50-E55. doi: 10.9778/cmajo.20200300. Print 2022 Jan-Mar. CMAJ Open. 2022. PMID: 35078823 Free PMC article.
-
Association of neighbourhood-level material deprivation with adverse outcomes and processes of care among patients with heart failure in a single-payer healthcare system: A population-based cohort study.Eur J Heart Fail. 2023 Dec;25(12):2274-2286. doi: 10.1002/ejhf.3090. Epub 2023 Dec 20. Eur J Heart Fail. 2023. PMID: 37953731
-
Impact of a social prescribing intervention in North East England on adults with type 2 diabetes: the SPRING_NE multimethod study.Public Health Res (Southampt). 2023 Mar;11(2):1-185. doi: 10.3310/AQXC8219. Public Health Res (Southampt). 2023. PMID: 37254700
Cited by
-
Prevalence of depression in melasma: a systematic review and meta-analysis.Front Psychiatry. 2024 Jan 8;14:1276906. doi: 10.3389/fpsyt.2023.1276906. eCollection 2023. Front Psychiatry. 2024. PMID: 38260775 Free PMC article.
-
Association of Neighborhood Deprivation With Thrombolysis and Thrombectomy for Acute Stroke in a Health System With Universal Access.Neurology. 2023 Nov 27;101(22):e2215-e2222. doi: 10.1212/WNL.0000000000207924. Neurology. 2023. PMID: 37914415 Free PMC article.
-
Community Disadvantage Is Associated With More Severe Motor Symptoms in Parkinson Disease.Neurol Clin Pract. 2025 Aug;15(4):e200506. doi: 10.1212/CPJ.0000000000200506. Epub 2025 Jun 26. Neurol Clin Pract. 2025. PMID: 40584637 Free PMC article.
References
-
- Havranek EP, Mujahid MS, Barr DA, et al. . Social determinants of risk and outcomes for cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2015;132(9):873-898. - PubMed
-
- Chen R, Crichton S, McKevitt C, Rudd AG, Sheldenkar A, Wolfe CD. Association between socioeconomic deprivation and functional impairment after stroke: the South London Stroke Register. Stroke. 2015;46(3):800-805. - PubMed
-
- Cesaroni G, Agabiti N, Forastiere F, Perucci CA. Socioeconomic differences in stroke incidence and prognosis under a universal healthcare system. Stroke. 2009;40(8):2812-2819. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials