

Long-term risk of subsequent ipsilateral lesions after surgery with or without radiotherapy for ductal carcinoma in situ of the breast
- PMID: 34408284
- PMCID: PMC8575990
- DOI: 10.1038/s41416-021-01496-6
Long-term risk of subsequent ipsilateral lesions after surgery with or without radiotherapy for ductal carcinoma in situ of the breast
Abstract
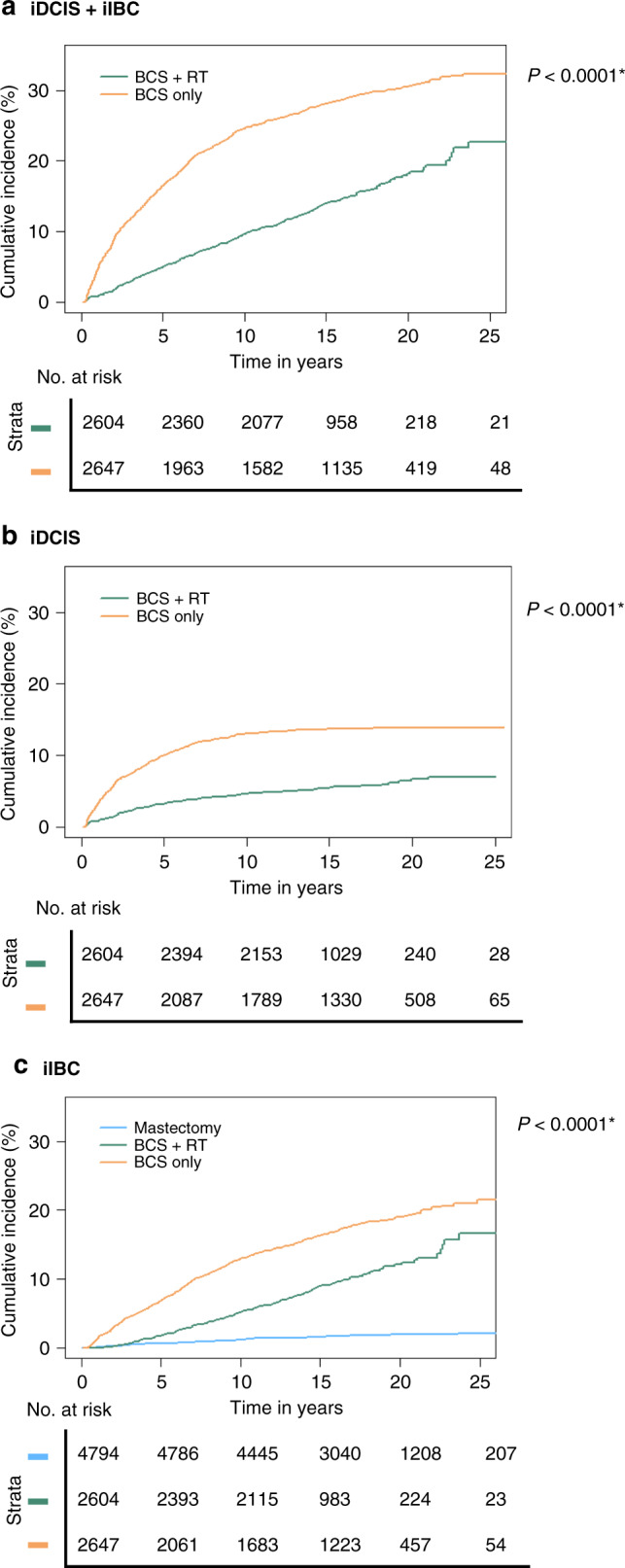
Background: Radiotherapy (RT) following breast-conserving surgery (BCS) for ductal carcinoma in situ (DCIS) reduces ipsilateral breast event rates in clinical trials. This study assessed the impact of DCIS treatment on a 20-year risk of ipsilateral DCIS (iDCIS) and ipsilateral invasive breast cancer (iIBC) in a population-based cohort.
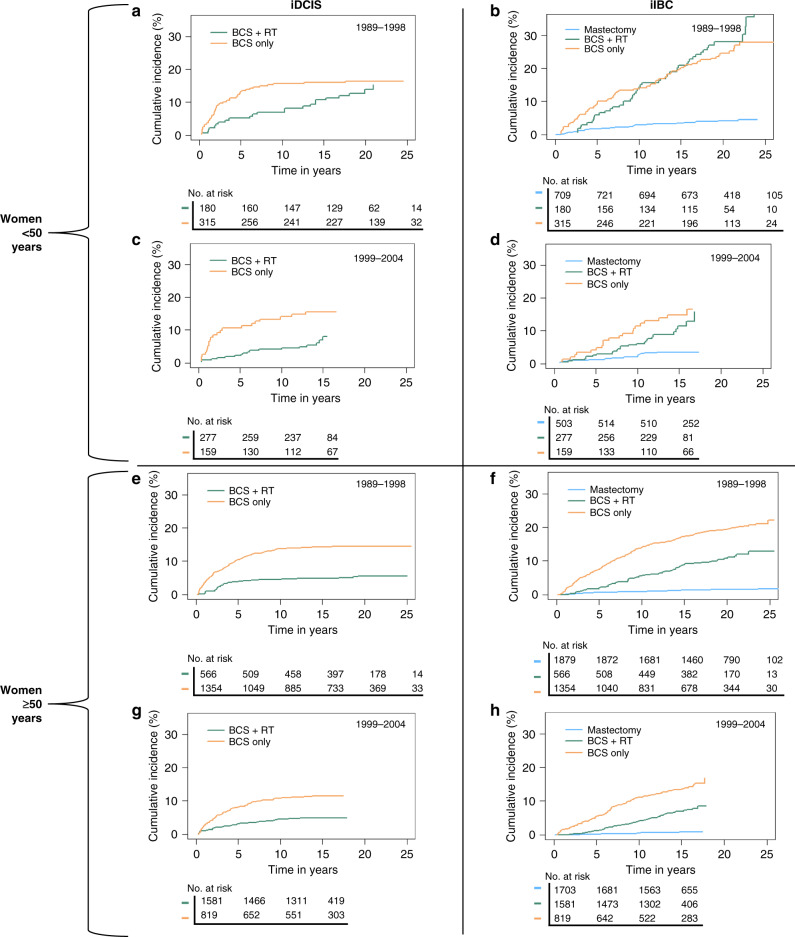
Methods: The cohort comprised all women diagnosed with DCIS in the Netherlands during 1989-2004 with follow-up until 2017. Cumulative incidence of iDCIS and iIBC following BCS and BCS + RT were assessed. Associations of DCIS treatment with iDCIS and iIBC risk were estimated in multivariable Cox models.
Results: The 20-year cumulative incidence of any ipsilateral breast event was 30.6% (95% confidence interval (CI): 28.9-32.6) after BCS compared to 18.2% (95% CI 16.3-20.3) following BCS + RT. Women treated with BCS compared to BCS + RT had higher risk of developing iDCIS and iIBC within 5 years after DCIS diagnosis (for iDCIS: hazard ratio (HR)age < 50 3.2 (95% CI 1.6-6.6); HRage ≥ 50 3.6 (95% CI 2.6-4.8) and for iIBC: HRage<50 2.1 (95% CI 1.4-3.2); HRage ≥ 50 4.3 (95% CI 3.0-6.0)). After 10 years, the risk of iDCIS and iIBC no longer differed for BCS versus BCS + RT (for iDCIS: HRage < 50 0.7 (95% CI 0.3-1.5); HRage ≥ 50 0.7 (95% CI 0.4-1.3) and for iIBC: HRage < 50 0.6 (95% CI 0.4-0.9); HRage ≥ 50 1.2 (95% CI 0.9-1.6)).
Conclusion: RT is associated with lower iDCIS and iIBC risk up to 10 years after BCS, but this effect wanes thereafter.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Netherlands Comprehensive Cancer Organisation (IKNL). DCIS incidence trends over time. The Netherlands. https://iknl.nl/nkr.
-
- Howlader N, Noone A, Krapcho M, Miller D, Brest A, Yu M, et al. SEER Cancer Statistics Review, 1975–2017. Bethesda: National Cancer Institute; 2017. https://seer.cancer.gov/csr/1975_2017/.
-
- Fisher B, Dignam J, Wolmark N, Mamounas E, Costantino J, Poller W, et al. Lumpectomy and radiation therapy for the treatment of intraductal breast cancer: findings from National Surgical Adjuvant Breast and Bowel Project B-17. J Clin Oncol. 1998;16:441–52. doi: 10.1200/JCO.1998.16.2.441. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
