

Association of Lymphocyte to Monocyte Ratio and Risk of in-Hospital Mortality in Patients with Cardiogenic Shock: A Propensity Score Matching Study
- PMID: 34408483
- PMCID: PMC8367081
- DOI: 10.2147/IJGM.S325907
Association of Lymphocyte to Monocyte Ratio and Risk of in-Hospital Mortality in Patients with Cardiogenic Shock: A Propensity Score Matching Study
Abstract
Background: Lymphocyte to monocyte ratio (LMR) has been long implicated in the prediction of many inflammatory-related diseases. However, the possible value as prognostic marker of LMR have not been evaluated in cardiogenic shock (CS) patients. The aim of the study was to assess the relationship between LMR on admission and in-hospital mortality in CS patients.
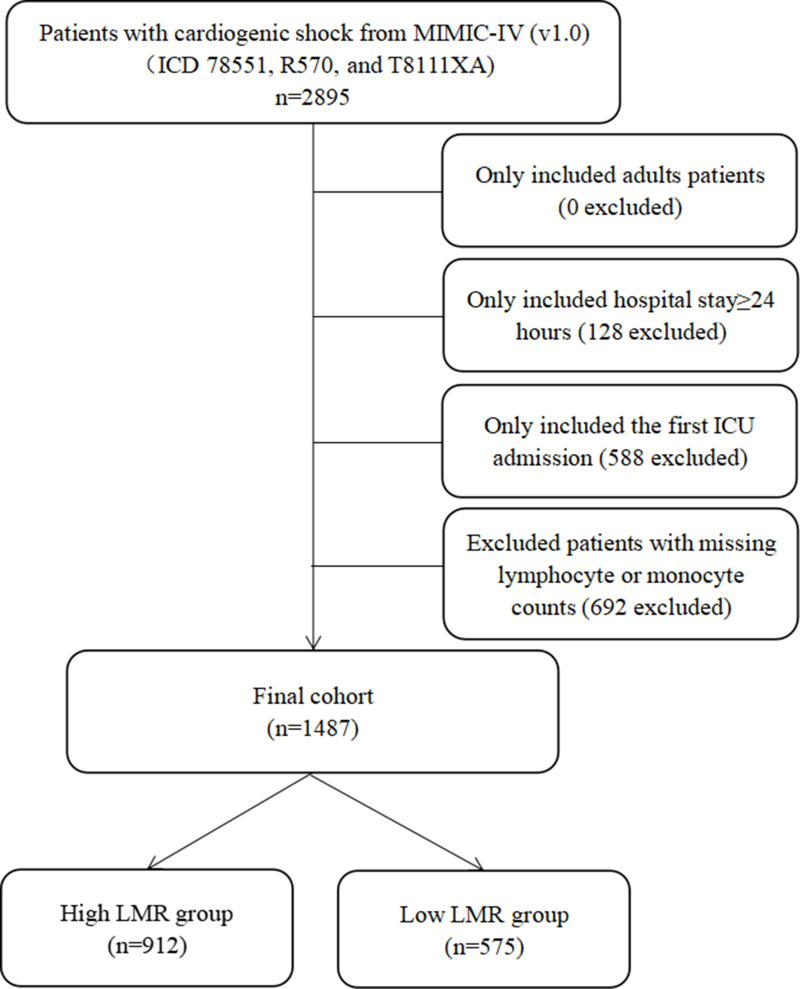
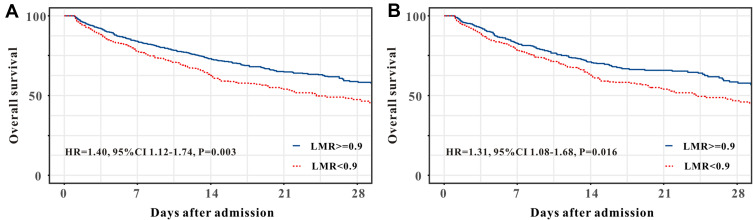
Methods: Data on patients diagnosed with CS were extracted from the Medical Information Mart for Intensive Care-IV (MIMIC-IV) database. We performed a single-institution, retrospective study of 1487 CS patients and determined the optimal cut-off for LMR by X-tile software. Propensity score matching (PSM) and inverse probabilities of treatment weighting (IPTW) were conducted to control confounders. Cox proportional hazards model was performed to evaluate the relationship between LMR and in-hospital mortality. Kaplan-Meier curves and receiver operating characteristics (ROC) analysis were applied to assess the prognostic value of LMR.
Results: The optimal cut-off value for LMR was 0.9. Cox proportional hazards model demonstrated that lower LMR (< 0.9) was independently associated with in-hospital mortality with hazard ratio (HR) of 1.40 (1.12-1.74, P = 0.003). The results were consistent with survival analyses (P < 0.001, Log rank test). Adding LMR< 0.9 to the sequential organ failure assessment (SOFA) score improved discrimination and risk stratification for in-hospital mortality.
Conclusion: Lower level of LMR is related to higher risk of in-hospital mortality of patients with CS. As an easily available biomarker, LMR can independently predict the in-hospital mortality in CS patients.
Keywords: CS; LMR; cardiogenic shock; lymphocyte to monocyte ratio; mortality.
© 2021 Zhang et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
The prognostic value of admission lymphocyte-to-monocyte ratio in critically ill patients with acute myocardial infarction.BMC Cardiovasc Disord. 2022 Jul 7;22(1):308. doi: 10.1186/s12872-022-02745-z. BMC Cardiovasc Disord. 2022. PMID: 35799102 Free PMC article.
-
Preoperative Lymphocyte-to-Monocyte Ratio as a Prognostic Predictor of Long-Term Mortality in Cardiac Surgery Patients: A Propensity Score Matching Analysis.Front Cardiovasc Med. 2021 Feb 22;8:639890. doi: 10.3389/fcvm.2021.639890. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 33693038 Free PMC article.
-
Predictive value of lymphocyte-to-monocyte ratio in critically Ill patients with atrial fibrillation: A propensity score matching analysis.J Clin Lab Anal. 2022 Feb;36(2):e24217. doi: 10.1002/jcla.24217. Epub 2021 Dec 30. J Clin Lab Anal. 2022. PMID: 34970783 Free PMC article.
-
Prognostic value of neutrophil-lymphocyte ratio in critically ill patients with cancer: a propensity score matching study.Clin Transl Oncol. 2021 Jan;23(1):139-147. doi: 10.1007/s12094-020-02405-8. Epub 2020 May 29. Clin Transl Oncol. 2021. PMID: 32472452
-
Predictive Value of a Prognostic Model Based on Lymphocyte-to-Monocyte Ratio Before Radioiodine Therapy for Recurrence of Papillary Thyroid Carcinoma.Technol Cancer Res Treat. 2021 Jan-Dec;20:15330338211027910. doi: 10.1177/15330338211027910. Technol Cancer Res Treat. 2021. PMID: 34191658 Free PMC article.
Cited by
-
SCAI Staging Application for Acute Myocardial Infarction-Related Cardiogenic Shock at a Single-Center Russian Registry.J Clin Med. 2023 Dec 17;12(24):7739. doi: 10.3390/jcm12247739. J Clin Med. 2023. PMID: 38137809 Free PMC article.
-
Predicting cardiovascular disease and all-cause mortality using the lymphocyte-to-monocyte ratio: Insights from explainable machine learning models.Int J Cardiol Cardiovasc Risk Prev. 2025 Jan 28;24:200372. doi: 10.1016/j.ijcrp.2025.200372. eCollection 2025 Mar. Int J Cardiol Cardiovasc Risk Prev. 2025. PMID: 39995422 Free PMC article.
-
The best of both worlds: no apparent trade-off between immunity and reproduction in two group-living African mole-rat species.Philos Trans R Soc Lond B Biol Sci. 2023 Aug 14;378(1883):20220310. doi: 10.1098/rstb.2022.0310. Epub 2023 Jun 26. Philos Trans R Soc Lond B Biol Sci. 2023. PMID: 37381852 Free PMC article.
-
Reduced IFN-γ levels along with changes in hematologic and immunologic parameters are key to COVID-19 severity in Bangladeshi patients.Exp Hematol. 2023 Feb;118:53-64.e1. doi: 10.1016/j.exphem.2022.11.006. Epub 2022 Nov 28. Exp Hematol. 2023. PMID: 36574579 Free PMC article.
-
Risk factors and an interpretability tool of in-hospital mortality in critically ill patients with acute myocardial infarction.Clin Med (Lond). 2025 May;25(3):100299. doi: 10.1016/j.clinme.2025.100299. Epub 2025 Feb 27. Clin Med (Lond). 2025. PMID: 40023290 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
