

Endoscopic treatment for gastric antral vascular ectasia
- PMID: 34408826
- PMCID: PMC8366108
- DOI: 10.1177/20406223211039696
Endoscopic treatment for gastric antral vascular ectasia
Abstract
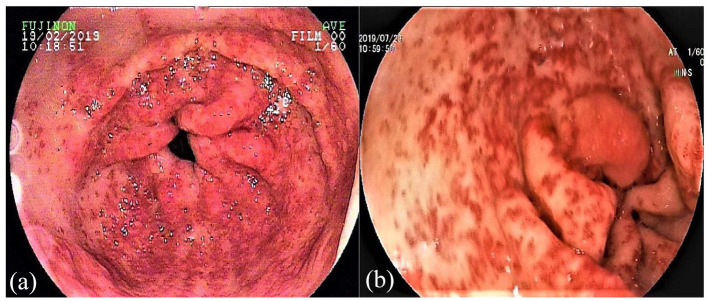
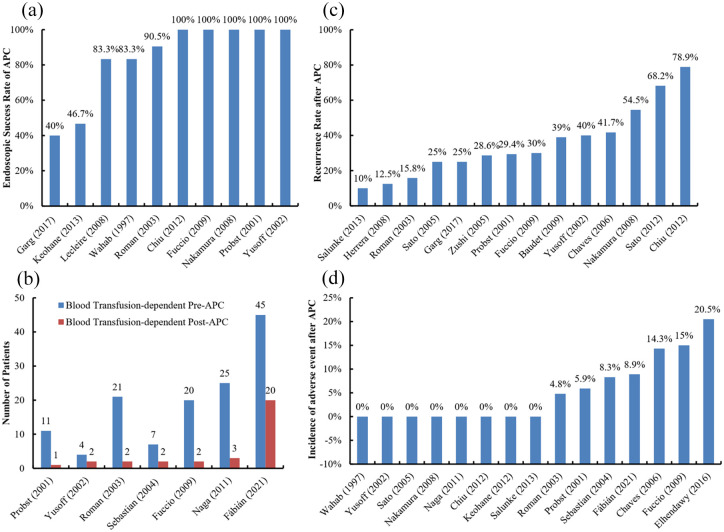
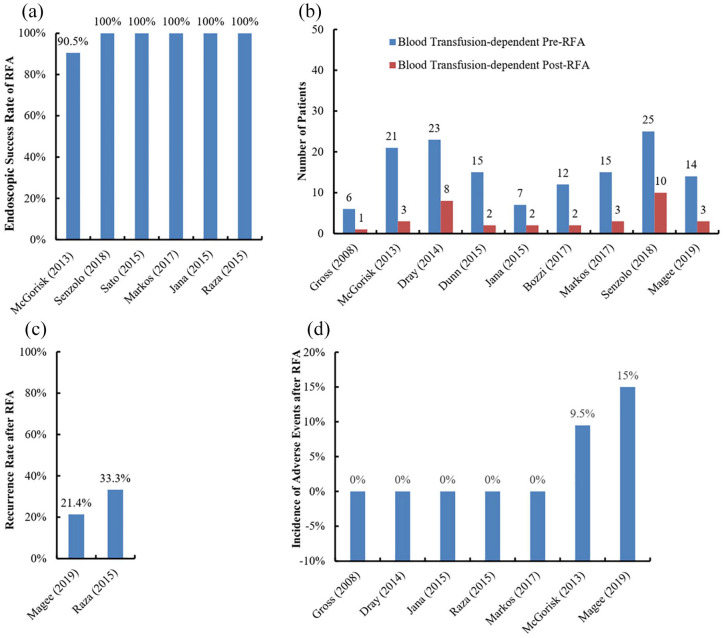
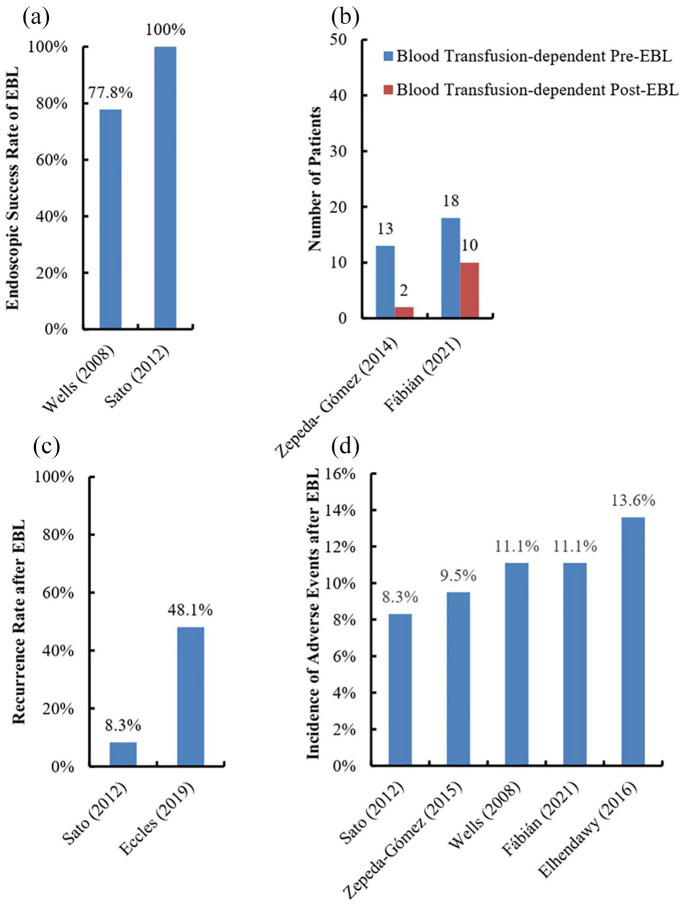
Gastric antral vascular ectasia (GAVE) is one of the uncommon causes of upper gastrointestinal bleeding. Major treatment of GAVE includes pharmacotherapy, endoscopy, and surgery. The efficacy and safety of pharmacotherapy have not been sufficiently confirmed; and surgery is just considered when conservative treatment is ineffective. By comparison, endoscopy is a common treatment option for GAVE. This paper reviews the currently used endoscopic approaches for GAVE, mainly including argon plasma coagulation (APC), radiofrequency ablation (RFA), and endoscopic band ligation (EBL). It also summarizes their efficacy and procedure-related adverse events. The endoscopic success rate of APC is 40-100%; however, APC needs several treatment sessions, with a high recurrence rate of 10-78.9%. The endoscopic success rates of RFA and EBL are 90-100% and 77.8-100%, respectively; and their recurrence rates are 21.4-33.3% and 8.3-48.1%, respectively. Hyperplastic gastric polyps and sepsis are major adverse events of APC and RFA; and Mallory-Weiss syndrome is occasionally observed after APC. Adverse events of EBL are rare and mild, such as nausea, vomiting, esophageal or abdominal pain, and hyperplastic polyps. APC is often considered as the first-line choice of endoscopic treatment for GAVE. RFA and EBL have been increasingly used as alternatives in patients with refractory GAVE. A high recurrence of GAVE after endoscopic treatment should be fully recognized and cautiously managed by follow-up endoscopy. In future, a head-to-head comparison of different endoscopic approaches for GAVE is warranted.
Keywords: argon plasma coagulation; endoscopic band ligation; gastric antral vascular ectasia; radiofrequency ablation.
© The Author(s), 2021.
Conflict of interest statement
Conflict of interest statement: The authors declare that there is no conflict of interest.
Figures
References
-
- Rider JA, Klotz AP, Kirsner JB.Gastritis with veno-capillary ectasia as a source of massive gastric hemorrhage. Gastroenterology 1953; 24: 118–123. - PubMed
-
- Jabbari M, Cherry R, Lough JO, et al. Gastric antral vascular ectasia: the watermelon stomach. Gastroenterology 1984; 87: 1165–1170. - PubMed
-
- Suit PF, Petras RE, Bauer TW, et al. Gastric antral vascular ectasia. A histologic and morphometric study of “the watermelon stomach”. Am J Surg Pathol 1987; 11: 750–757. - PubMed
-
- Saperas E, Perez Ayuso RM, Poca E, et al. Increased gastric PGE2 biosynthesis in cirrhotic patients with gastric vascular ectasia. Am J Gastroenterol 1990; 85: 138–144. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
