

The spectrum of clinical sequelae associated with alpha-1 antitrypsin deficiency
- PMID: 34408829
- PMCID: PMC8367210
- DOI: 10.1177/2040622321995691
The spectrum of clinical sequelae associated with alpha-1 antitrypsin deficiency
Abstract
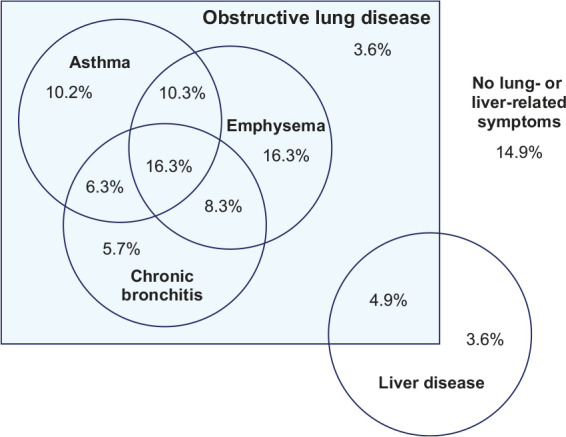
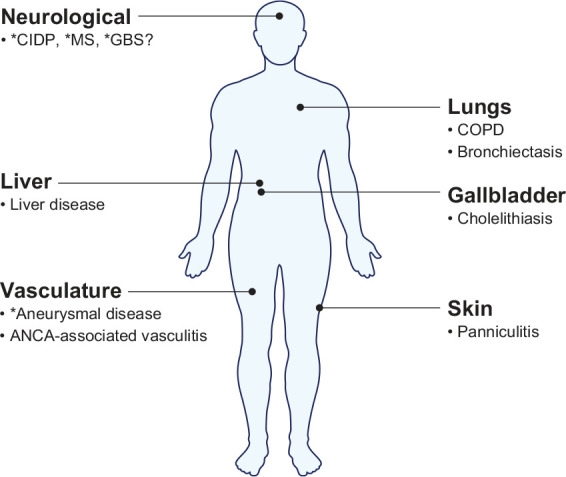
Alpha-1 antitrypsin (AAT) deficiency (AATD) is an autosomal co-dominant condition that predisposes to the development of lung disease, primarily emphysema. Emphysema results from the breakdown of lung matrix elastin by proteases, including neutrophil elastase, a protease normally inhibited by AAT. AATD also predisposes to liver (cirrhosis) and skin (panniculitis) disease, and to vasculitis. The prevalence of AATD is estimated to be approximately 1 in 3,500 individuals in the United States. However, lack of awareness of AATD among some physicians, misperceptions regarding the absence of effective therapy, and the close overlap in symptoms with asthma and non-AATD chronic obstructive pulmonary disease are thought to contribute to under-recognition of the disease. In patients with AATD, treatment with intravenous AAT augmentation therapy is the only currently available treatment known to slow the progression of emphysema. Moreover, smoking cessation and other lifestyle interventions also help improve outcomes. Early diagnosis and intervention are of key importance due to the irreversible nature of the resultant emphysema. Liver disease is the second leading cause of death among patients with AATD and a minority of patients present with panniculitis or antineutrophil cytoplasmic antibody-associated vasculitis, thought to be directly related to AATD. Though no randomized trial has assessed the effectiveness of augmentation therapy for AATD-associated panniculitis, clinical experience and case series suggest there is a benefit. Other diseases putatively linked to AATD include aneurysmal disease and multiple neurological conditions, although these associations remain speculative in nature.
Keywords: Alpha-1 antitrypsin; Alpha-1 antitrypsin deficiency; antineutrophil cytoplasmic antibody-associated vasculitis; chronic obstructive pulmonary disease; emphysema; panniculitis.
© The Author(s), 2021.
Conflict of interest statement
Conflict of interest statement: JKS reports serving as a consultant to Grifols, Takeda, CSL Behring, 23andMe, Insmed, Vertex, InhibRx, Dicerna and Arrowhead Pharmaceuticals. VT reports no conflicts of interest.
Figures
References
-
- American Thoracic Society and European Respiratory Society. American Thoracic Society/European Respiratory Society statement: standards for the diagnosis and management of individuals with alpha-1 antitrypsin deficiency. Am J Respir Crit Care Med 2003; 168: 818–900. - PubMed
-
- Miravitlles M, Dirksen A, Ferrarotti I, et al. European Respiratory Society statement: diagnosis and treatment of pulmonary disease in alpha1-antitrypsin deficiency. Eur Respir J 2017; 50: 1700610. - PubMed
-
- Stoller JK, Aboussouan LS.A review of α1-antitrypsin deficiency. Am J Respir Crit Care Med 2012; 185: 246–259. - PubMed
-
- Hatipoğlu U, Stoller JK.α1-Antitrypsin deficiency. Clin Chest Med 2016; 37: 487–504. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
