

Current strategies for managing chronic thromboembolic pulmonary hypertension: results of the worldwide prospective CTEPH Registry
- PMID: 34409094
- PMCID: PMC8365143
- DOI: 10.1183/23120541.00850-2020
Current strategies for managing chronic thromboembolic pulmonary hypertension: results of the worldwide prospective CTEPH Registry
Abstract
Background: Pulmonary endarterectomy (PEA), pulmonary arterial hypertension (PAH) therapy and balloon pulmonary angioplasty (BPA) are currently accepted therapies for chronic thromboembolic pulmonary hypertension (CTEPH). This international CTEPH Registry identifies clinical characteristics of patients, diagnostic algorithms and treatment decisions in a global context.
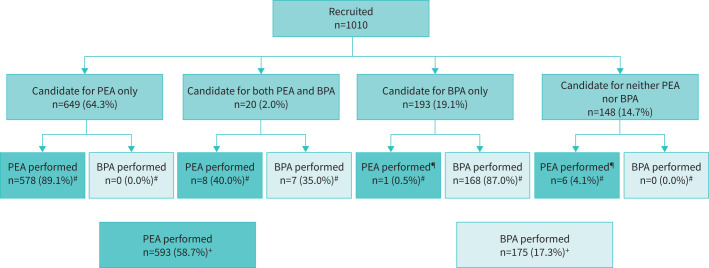
Methods: 1010 newly diagnosed consecutive patients were included in the registry between February 2015 and September 2016. Diagnosis was confirmed by right heart catheterisation, ventilation-perfusion lung scan, computerised pulmonary angiography and/or invasive pulmonary angiography after at least 3 months on anticoagulation.
Results: Overall, 649 patients (64.3%) were considered for PEA, 193 (19.1%) for BPA, 20 (2.0%) for both PEA and BPA, and 148 (14.7%) for PAH therapy only. Reasons for PEA inoperability were technical inaccessibility (n=235), comorbidities (n=63) and patient refusal (n=44). In Europe and America and other countries (AAO), 72% of patients were deemed suitable for PEA, whereas in Japan, 70% of patients were offered BPA as first choice. Sex was evenly balanced, except in Japan where 75% of patients were female. A history of acute pulmonary embolism was reported for 65.6% of patients. At least one PAH therapy was initiated in 35.8% of patients (26.2% of PEA candidates, 54.5% of BPA candidates and 54.1% of those not eligible for either PEA or BPA). At the time of analysis, 39 patients (3.9%) had died of pulmonary hypertension-related causes (3.5% after PEA and 1.8% after BPA).
Conclusions: The registry revealed noticeable differences in patient characteristics (rates of pulmonary embolism and sex) and therapeutic approaches in Japan compared with Europe and AAO.
Copyright ©The authors 2021.
Conflict of interest statement
Conflict of interest: S. Guth reports personal fees from Actelion, Bayer, GSK, MSD and Pfizer outside the submitted work. Conflict of interest: A.M. D'Armini reports personal fees from Actelion, Bayer and MSD outside the submitted work. Conflict of interest: M. Delcroix reports grants and personal fees from Actelion, and personal fees from Bayer, MSD, Reata and Bellarophon, outside the submitted work. Conflict of interest: K. Nakayama has nothing to disclose. Conflict of interest: E. Fadel has nothing to disclose. Conflict of interest: S.P. Hoole has nothing to disclose. Conflict of interest: D.P. Jenkins reports personal fees from Actelion, and grants and personal fees from Bayer, outside the submitted work. Conflict of interest: D.G. Kiely reports grants, personal fees and nonfinancial support from Actelion, Bayer and GSK, and personal fees and nonfinancial support from MSD, outside the submitted work. Conflict of interest: N.H. Kim reports personal fees from Actelion, Bayer and Merck, and grants from United Therapeutics and SoniVie, outside the submitted work. Conflict of interest: I.M. Lang reports grants and personal fees from Actelion and AOPOrphan Pharma, personal fees from MSD, and nonfinancial support from Medtronic, during the conduct of the study; and grants and personal fees from Actelion and AOPOrphan, and personal fees from MSD and Ferrer, outside the submitted work. Conflict of interest: M.M. Madani is a consultant for Actelion. Conflict of interest: H. Matsubara reports personal fees from Actelion, AOP orphan Pharmaceuticals AG, Bayer, GlaxoSmithKline, Pfizer Japan, Inc., United Therapeutics, Nippon Shinyaku, Co., Ltd, and Kaneka Medix Corporation, outside the submitted work. Conflict of interest: A. Ogawa reports personal fees from Nippon Shinyaku Co., Ltd., outside the submitted work. Conflict of interest: J. Ota-Arakaki has nothing to disclose. Conflict of interest: R. Quarck has nothing to disclose. Conflict of interest: R. Sadushi-Kolici has nothing to disclose. Conflict of interest: G. Simonneau has nothing to disclose. Conflict of interest: C.B. Wiedenroth reports personal fees from Actelion, AOP, Bayer, MSD and Pfizer outside the submitted work. Conflict of interest: B. Yildizeli has nothing to disclose. Conflict of interest: E. Mayer reports personal fees from Actelion, Bayer, MSD and BMS outside the submitted work. Conflict of interest: J. Pepke-Zaba reports personal fees and nonfinancial support from Actelion and Merck, and nonfinancial support from GSK, outside the submitted work.
Figures
References
LinkOut - more resources
Full Text Sources
Medical