

Spectrum, risk factors and outcomes of neurological and psychiatric complications of COVID-19: a UK-wide cross-sectional surveillance study
- PMID: 34409289
- PMCID: PMC8364668
- DOI: 10.1093/braincomms/fcab168
Spectrum, risk factors and outcomes of neurological and psychiatric complications of COVID-19: a UK-wide cross-sectional surveillance study
Abstract
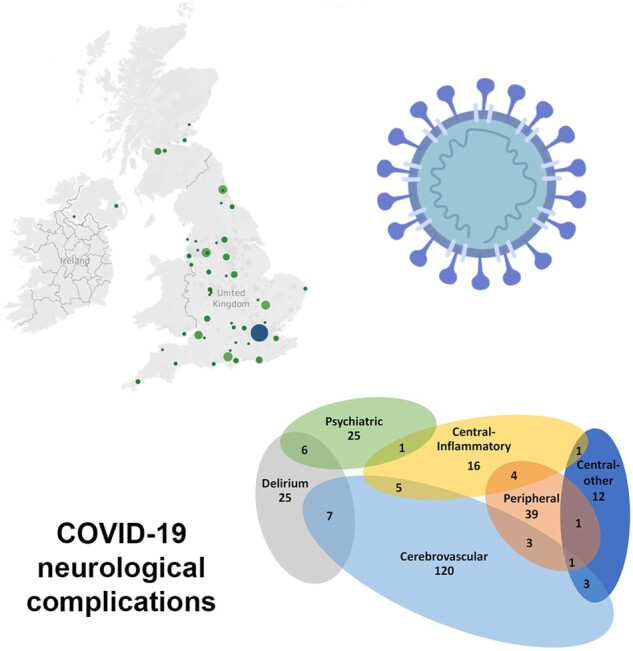
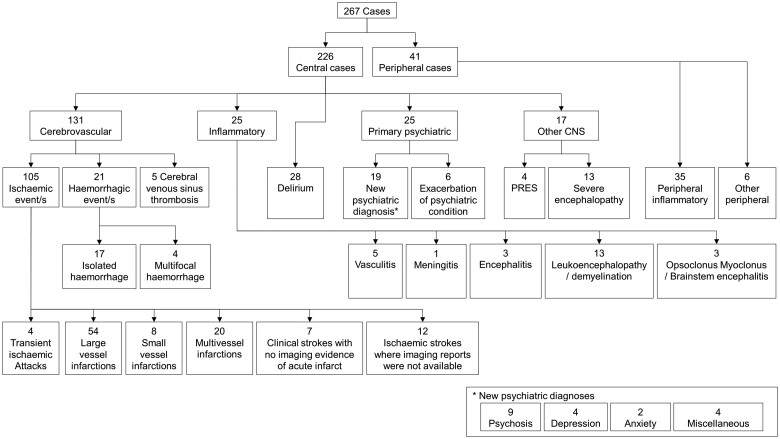
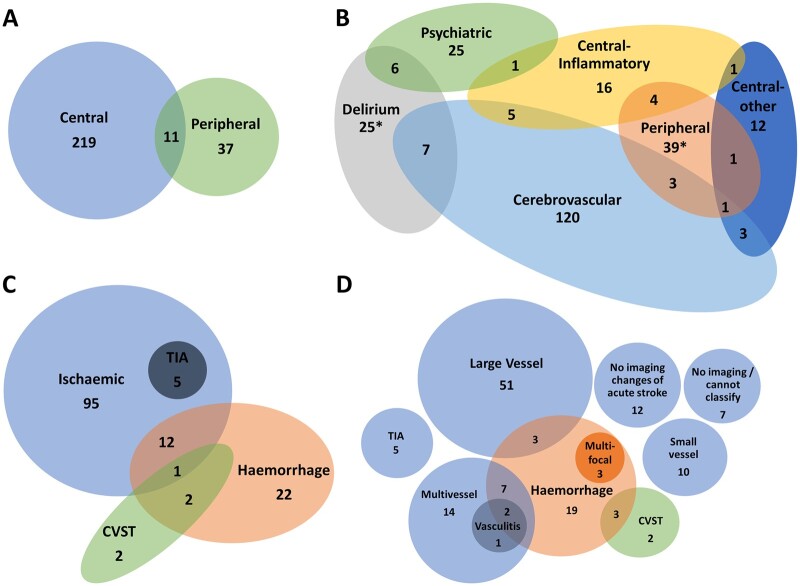
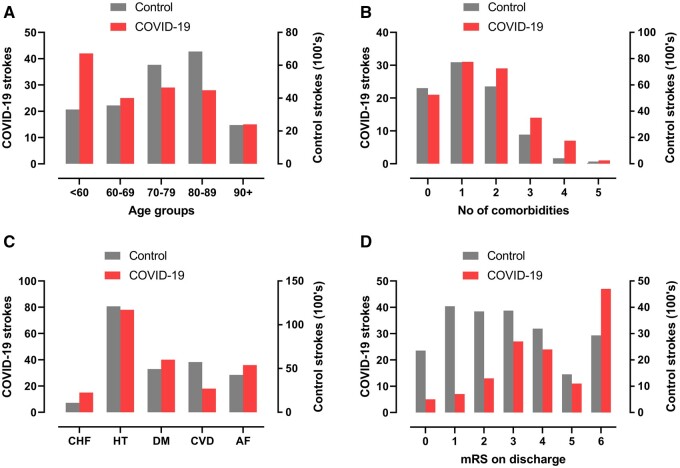
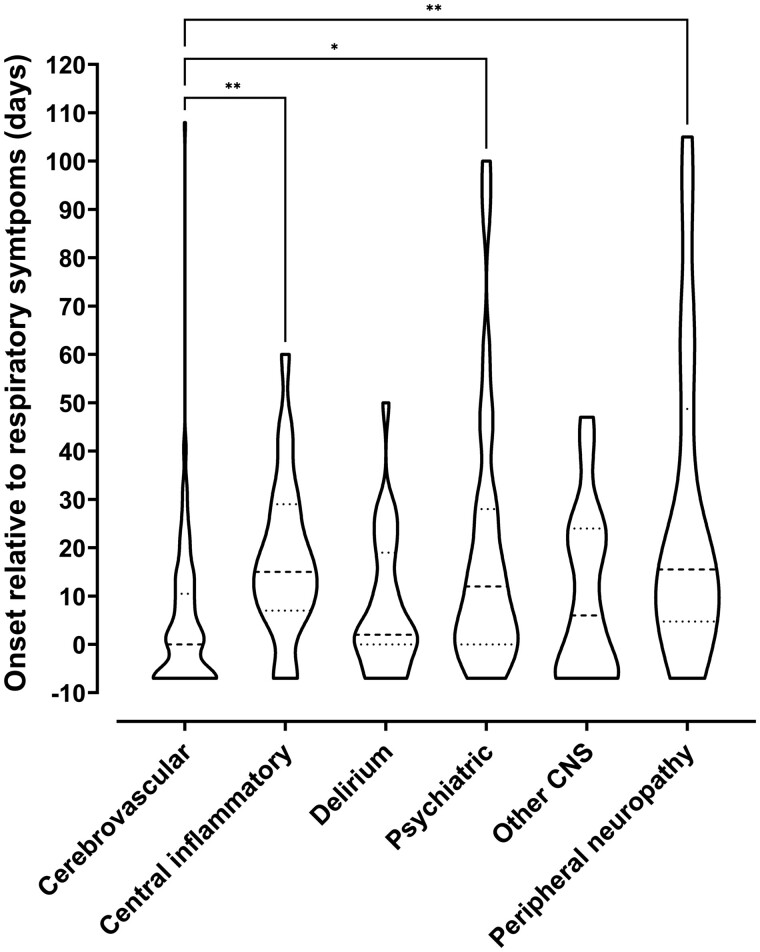
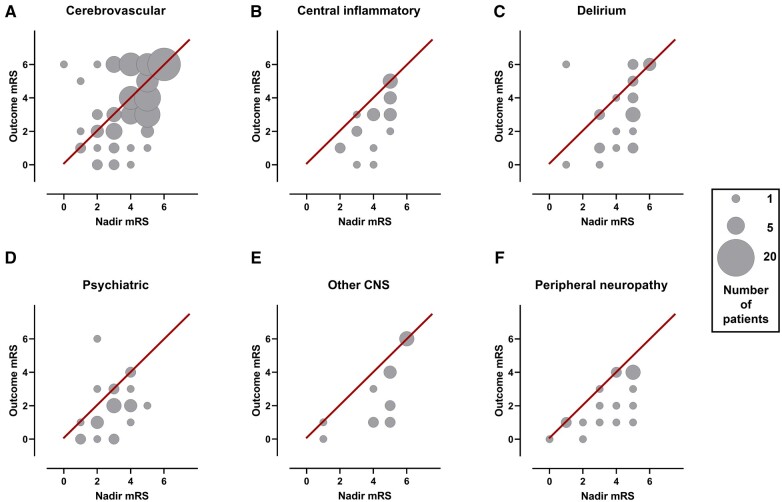
SARS-CoV-2 is associated with new-onset neurological and psychiatric conditions. Detailed clinical data, including factors associated with recovery, are lacking, hampering prediction modelling and targeted therapeutic interventions. In a UK-wide cross-sectional surveillance study of adult hospitalized patients during the first COVID-19 wave, with multi-professional input from general and sub-specialty neurologists, psychiatrists, stroke physicians, and intensivists, we captured detailed data on demographics, risk factors, pre-COVID-19 Rockwood frailty score, comorbidities, neurological presentation and outcome. A priori clinical case definitions were used, with cross-specialty independent adjudication for discrepant cases. Multivariable logistic regression was performed using demographic and clinical variables, to determine the factors associated with outcome. A total of 267 cases were included. Cerebrovascular events were most frequently reported (131, 49%), followed by other central disorders (95, 36%) including delirium (28, 11%), central inflammatory (25, 9%), psychiatric (25, 9%), and other encephalopathies (17, 7%), including a severe encephalopathy (n = 13) not meeting delirium criteria; and peripheral nerve disorders (41, 15%). Those with the severe encephalopathy, in comparison to delirium, were younger, had higher rates of admission to intensive care and a longer duration of ventilation. Compared to normative data during the equivalent time period prior to the pandemic, cases of stroke in association with COVID-19 were younger and had a greater number of conventional, modifiable cerebrovascular risk factors. Twenty-seven per cent of strokes occurred in patients <60 years. Relative to those >60 years old, the younger stroke patients presented with delayed onset from respiratory symptoms, higher rates of multi-vessel occlusion (31%) and systemic thrombotic events. Clinical outcomes varied between disease groups, with cerebrovascular disease conferring the worst prognosis, but this effect was less marked than the pre-morbid factors of older age and a higher pre-COVID-19 frailty score, and a high admission white cell count, which were independently associated with a poor outcome. In summary, this study describes the spectrum of neurological and psychiatric conditions associated with COVID-19. In addition, we identify a severe COVID-19 encephalopathy atypical for delirium, and a phenotype of COVID-19 associated stroke in younger adults with a tendency for multiple infarcts and systemic thromboses. These clinical data will be useful to inform mechanistic studies and stratification of patients in clinical trials.
Keywords: COVID-19; SARS-CoV-2; encephalopathy; neurology; stroke.
© The Author(s) (2021). Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
References
Grants and funding
- G108/613/MRC_/Medical Research Council/United Kingdom
- MR/V007181/1/MRC_/Medical Research Council/United Kingdom
- MC_UU_12023/23/MRC_/Medical Research Council/United Kingdom
- G1002605/MRC_/Medical Research Council/United Kingdom
- MR/W006251/1/MRC_/Medical Research Council/United Kingdom
- WT_/Wellcome Trust/United Kingdom
- MR/V03605X/1/MRC_/Medical Research Council/United Kingdom
- TURNER/OCT18/989-797/MNDA_/Motor Neurone Disease Association/United Kingdom
- MC_UU_12023/26/MRC_/Medical Research Council/United Kingdom
- MR/T028750/1/MRC_/Medical Research Council/United Kingdom
- MC_UU_00004/04/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Miscellaneous