

Impact of Risk and Volume on Procedural Traning of Pulmonary and Critical Care Fellows
- PMID: 34409416
- PMCID: PMC8362760
- DOI: 10.34197/ats-scholar.2020-0110OC
Impact of Risk and Volume on Procedural Traning of Pulmonary and Critical Care Fellows
Abstract
Background: Invasive procedures are a core aspect of pulmonary and critical care practice. Procedures performed in the intensive care unit can be divided into high-risk, low-volume (HRLV) procedures and low-risk, high-volume (LRHV) procedures. HRLV procedures include cricothyroidotomy, pericardiocentesis, Blakemore tube placement, and bronchial blocker placement. LRHV procedures include arterial line placement, central venous catheter placement, thoracentesis, and flexible bronchoscopy. Despite the frequency and importance of procedures in critical care medicine, little is known about the similarities and differences in procedural training between different Pulmonary and Critical Care Medicine (PCCM) and Critical Care Medicine (CCM) training programs. Furthermore, differences in procedural training practices for HRLV and LRHV procedures have not previously been described.
Objective: To assess procedural training practices in PCCM and CCM fellowship programs in the United States, and compare differences in training between HRLV and LRHV procedures.
Methods: A novel survey instrument was developed and disseminated to PCCM and CCM program directors and associate program directors at PCCM and CCM fellowship programs in the United States to assess procedural teaching practices for HRLV and LRHV procedures.
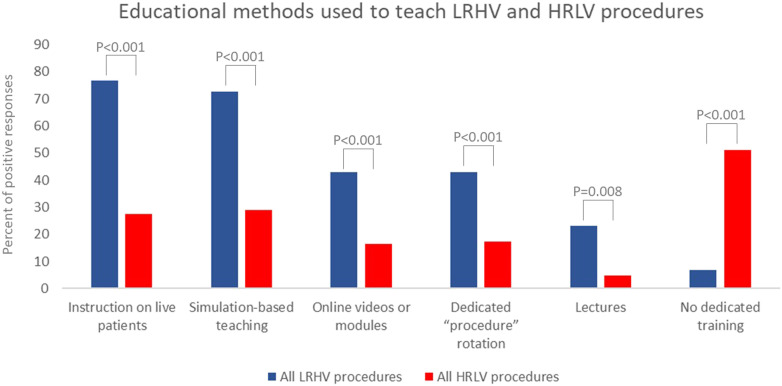
Results: The survey was sent to 221 fellowship programs, 168 PCCM and 34 CCM, with 70 unique respondents (31.7% response rate). Of the procedural educational strategies assessed, each strategy was used significantly more frequently for LRHV versus HRLV procedures. The majority of respondents (51.1%) report having no dedicated training for HRLV procedures versus 6.9% reporting no dedicated training for any LRHV procedure (P < 0.001). For HRLV procedures, 76.9% of respondents indicated that there was no set number of procedures required to determine competency, versus 25.3% for LRHV procedures (P < 0.001). For LRHV procedures, fellows were allowed to perform procedures independently without supervision 21.7% of the time versus 3.9% for HRLV procedures (P = 0.004). Program directors' confidence in their ability to determine fellows' competence in performing procedures was significantly lower for HRLV versus LRHV versus HRLV procedures (P < 0.001).
Conclusion: Significant differences exist in procedural training education for PCCM and CCM fellows for LRHV versus HRLV procedures, and awareness of this discrepancy presents an opportunity to address this educational gap in PCCM and CCM fellowship training.
Keywords: critical care; graduate medical education; risk evaluation and mitigation; teaching.
Copyright © 2021 by the American Thoracic Society.
Figures
Comment in
References
-
- American Board of Internal Medicine. Philadelphia, PA: American Board of Internal Medicine; 2020. Internal medicine certification policies. [accessed 2020 Jul 20]. Available from: https://www.abim.org/certification/policies/internal-medicine-subspecial....
-
- Accreditation Council for Graduate Medical Education, Common Program Requirements for Pulmonary and Critical Care Medicine Fellowship Programs. [accessed 2020 May 22]. Available from: https://www.acgme.org/What-We-Do/Accreditation/Common-Program-Requirements.
-
- Fessler HE, Addrizzo-Harris D, Beck JM, Buckley JD, Pastores SM, Piquette CA, et al. Entrustable professional activities and curricular milestones for fellowship training in pulmonary and critical care medicine: report of a multisociety working group. Chest. 2014;146:813–834. - PubMed
-
- Rothschild JM, Landrigan CP, Cronin JW, Kaushal R, Lockley SW, Burdick E, et al. The Critical Care Safety Study: the incidence and nature of adverse events and serious medical errors in intensive care. Crit Care Med. 2005;33:1694–1700. - PubMed
-
- Nilsson L, Pihl A, Tågsjö M, Ericsson E. Adverse events are common on the intensive care unit: results from a structured record review. Acta Anaesthesiol Scand. 2012;56:959–965. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
