

Photoreactive Hydrogel Stiffness Influences Volumetric Muscle Loss Repair
- PMID: 34409861
- PMCID: PMC9057873
- DOI: 10.1089/ten.TEA.2021.0137
Photoreactive Hydrogel Stiffness Influences Volumetric Muscle Loss Repair
Abstract
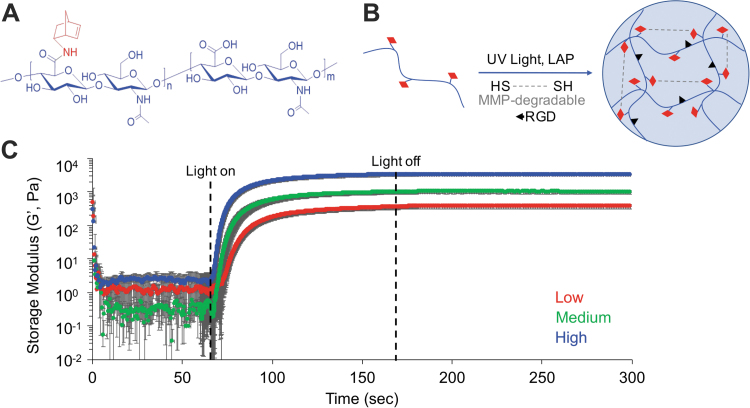
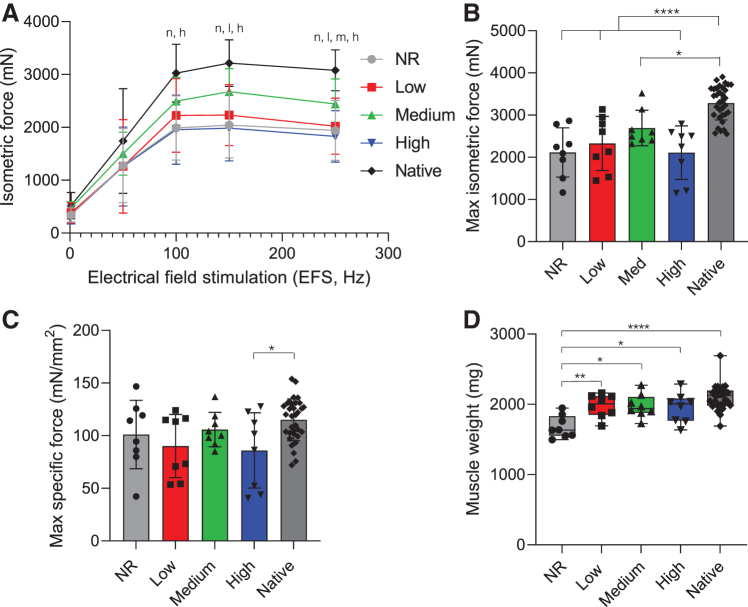
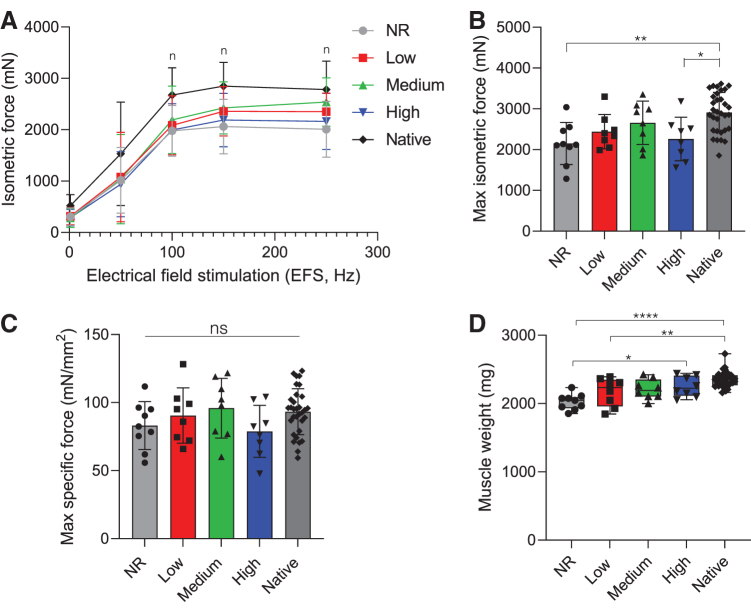
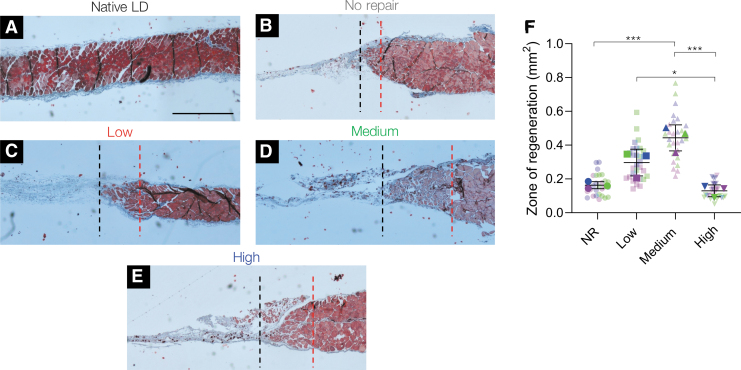
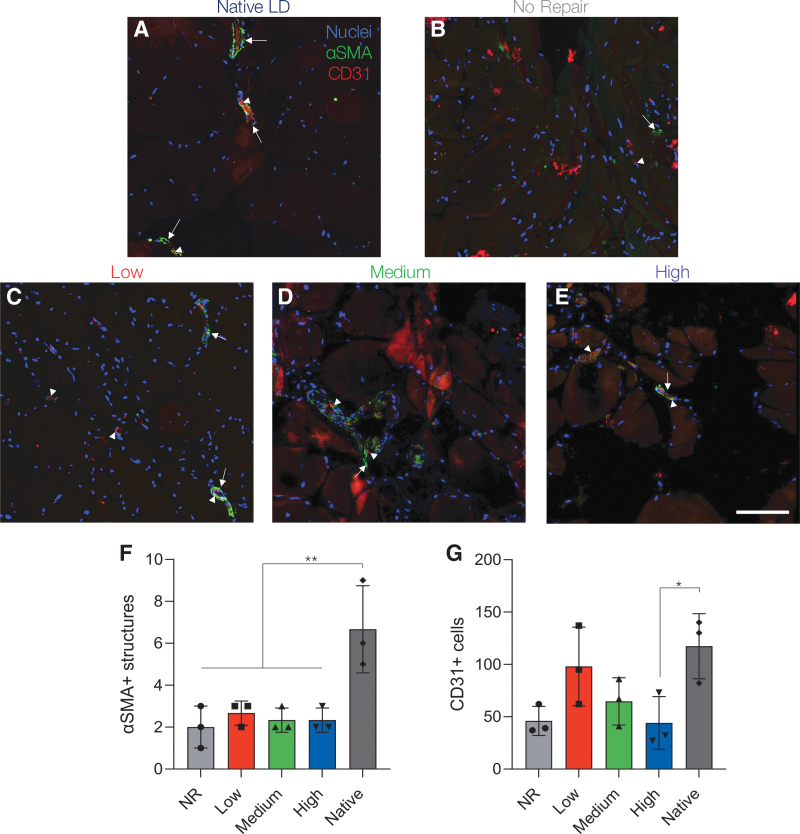
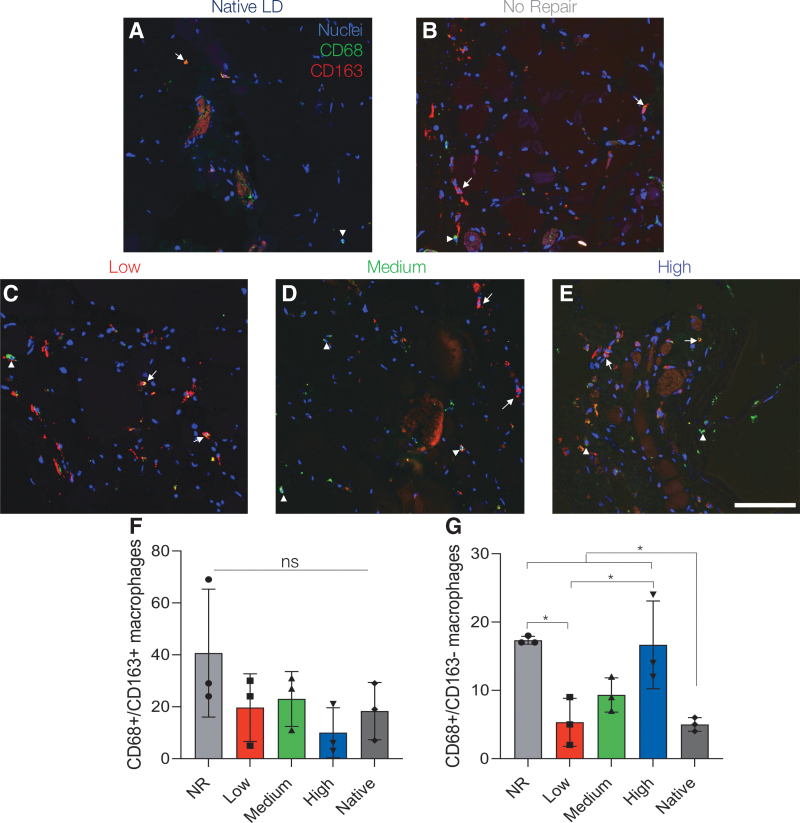
Volumetric muscle loss (VML) injuries are characterized by permanent loss of muscle mass, structure, and function. Hydrogel biomaterials provide an attractive platform for skeletal muscle tissue engineering due to the ability to easily modulate their biophysical and biochemical properties to match a range of tissue characteristics. In this work, we successfully developed a mechanically tunable hyaluronic acid (HA) hydrogel system to investigate the influence of hydrogel stiffness on VML repair. HA was functionalized with photoreactive norbornene groups to create hydrogel networks that rapidly crosslink through thiol-ene click chemistry with tailored mechanics. Mechanical properties were controlled by modulating the amount of matrix metalloproteinase-degradable peptide crosslinker to produce hydrogels with increasing elastic moduli of 1.1 ± 0.002, 3.0 ± 0.002, and 10.6 ± 0.006 kPa, mimicking a relevant range of developing and mature muscle stiffnesses. Functional muscle recovery was assessed following implantation of the HA hydrogels by in situ photopolymerization into rat latissimus dorsi (LD) VML defects at 12 and 24 weeks postinjury. After 12 weeks, muscles treated with medium stiffness (3.0 kPa) hydrogels produced maximum isometric forces most similar to contralateral healthy LD muscles. This trend persisted at 24 weeks postinjury, suggestive of sustained functional recovery. Histological analysis revealed a significantly larger zone of regeneration with more de novo muscle fibers following implantation of medium stiffness hydrogels in VML-injured muscles compared to other experimental groups. Lower (low and medium) stiffness hydrogels also appeared to attenuate the chronic inflammatory response characteristic of VML injuries, displaying similar levels of macrophage infiltration and polarization to healthy muscle. Together these findings illustrate the importance of hydrogel mechanical properties in supporting functional repair of VML injuries. Impact statement This report defines the role hydrogel mechanical properties play in the repair of volumetric muscle loss (VML) injuries. We show that an intermediate hydrogel stiffness (3 kPa) more compliant than adult muscle tissue facilitated improved and sustained regenerative outcomes up to 24 weeks postinjury in a rat latissimus dorsi model of VML. Muscles treated with 3 kPa hydrogels showed enhanced myogenesis and attenuation of the chronic inflammatory response characteristic of VML injuries. These results should help guide the future design of hydrogels for skeletal muscle tissue engineering and regeneration.
Keywords: hydrogel; regenerative medicine; volumetric muscle loss.
Conflict of interest statement
No competing financial interests exist.
Figures


References
-
- Carlson, B., and Faulkner, J.. The regeneration of skeletal muscle fibers following injury: a review. Med Sci Sports Exerc 15, 187, 1983. - PubMed
-
- Gorgan, B., and Hsu, J.R.. Volumetric muscle loss. J Am Acad Orthop Surg 19, 35, 2011. - PubMed
-
- Goldberg, M.S. Death and injury rates of U.S. military personnel in Iraq. Mil Med 175, 220, 2010. - PubMed
-
- Corona, B.T., Rivera, J.C., Owens, J.G., Wenke, J.C., and Rathbone, C.R.. Volumetric muscle loss leads to permanent disability following extremity trauma. J Rehabil Res Dev 52, 785, 2015. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
